Key Points
- ▪
There have been few studies of the yield and contribution of CCT to the evaluation of infective endocarditis, but vegetations can be imaged, and several structural complications of endocarditis have been well described.
- ▪
The use of CCT to establish the absence of significant coronary artery disease in patients with complicated cases of aortic valve endocarditis who are to undergo surgery is appealing because it obviates the need for catheter-based coronary angiography.
- ▪
Fibroelastomas of the aortic valve also can be depicted by CCT.
Infectious Endocarditis
Although it is still early in the process of validating cardiac CT (CCT), this test may have a role to play in the assessment of aortic valve endocarditis—less to assess vegetations than to assess the aortic root for abscesses. The erratic oscillatory motion of many vegetations, and their irregular surfaces, render the lesions underrepresented, principally due to partial volume averaging effects.
Complications of endocarditis such as vegetations, abscesses, and fistulas can be imaged by CCT ( Table 18-1 ). Although cardiac MR (CMR) previously was better validated for the detection of root complications of endocarditis, current CCT technology appears considerably more promising. Root abscess lesions can be imaged by CCT if they are not seen by transesophageal echocardiography (TEE), but metallic prosthetic valve material may impart image artifact in the vicinity of a ring abscess. CMR suffers from the same effect, probably to a greater degree.
| SENSITIVITY (%) | SPECIFICITY (%) | PPV (%) | NPV (%) | INTERMODALITY AGREEMENT | |
|---|---|---|---|---|---|
| Valvular abnormalities | 97 | 98 | 97 | 88 | κ = 0.84 |
| Vegetations | 96 | ||||
| Abscesses | 100 | ||||
| Perforations ≤ 2 mm | 0 | ||||
| Mobility of vegetations | 96 | ||||
| Correlation of size versus TEE | r = 0.95, P < .001 | ||||
| Per-valve basis for the detection of vegetations, abscesses/ pseudoaneurysms | 96 | 97 | 96 | 97 | |
| TEE | 100 | 100 | 100 | 100 |
∗ n = 37 patients with suspected IE; TEE versus CCT, 29 cases proven to have definite IE
Transthoracic echocardiography (TTE) and TEE remain the principal tests for assessing the presence of vegetations, abscesses, and fistulas. These tests do have limitations, however, especially in the presence of aortic valve prostheses, where the prosthesis is imaged edge-on and the sewing ring, in particular, may acoustically shadow the far side structures or cover them in reverberation artifact, thus obscuring relevant findings. Minor degrees of perivalvular insufficiency, while commonly seen in endocarditis, are not specific for this condition. It may be difficult to distinguish postoperative inflammatory changes and hematomas from infectious changes by TEE and probably by any modality. When compared with surgical findings, incorrect echocardiographic diagnosis was found in 7% of mitral mechanical valve cases and in 15% of aortic valve mechanical prosthesis cases.
The predictive value of CCT for the diagnosis of all anatomic echocardiographic findings of endocarditis has been published ( Table 18-2 ).
| TRUE POSITIVES | FALSE POSITIVES | PPV (%) | |
|---|---|---|---|
| Vegetations | 17 | 1 | 94 |
| Abscesses | 19 | 1 | 96 |
| Dehiscences | 4 | 0 | 100 |
| Pseudoaneurysms | 3 | 0 | 100 |
| Fistulas | 2 | 0 | 100 |
| Perivalvular leaks | |||
| Mild regurgitation | 1 | 1 | 6 |
| Moderate to severe regurgitation | 15 | 0 | 100 |
| All echocardiographic findings | 61 | 16 | 94 |
Vegetations
Valvular vegetations can be imaged by CCT ( Figs. 18-1 through 18-5 ; ).





Structural Complications of Endocarditis
- □
Abscesses and fistulas can be imaged by CCT.
- □
For images of valvular endocarditic perforations, see Figures 18-6 through 18-8 ;

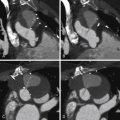
Figure 18-6
Oblique multiplanar reformatted images show a cross section through the aortic valve in the open position ( A ) and immediately below the valve in the closed position ( B ). C and D , The corresponding thin-slab three-dimensional (3D) volumetric reconstructions with the blood pool inverted to better display valvular anatomy. Note the functionally bicuspid valve in A and C. With the valve closed ( D ) there is clear delineation of the commissural fusion of the right and left cusps, the median raphe, and a 5-mm perforation of the noncoronary cusp, all best shown on the 3D volumetric reconstruction. E, Operative specimen showing a 5-mm perforation of the noncoronary cusp of the bicuspid aortic valve.Related posts:
 Overview of the Process, Exclusions and Risks, and Preparation
Overview of the Process, Exclusions and Risks, and Preparation
 CTA Assessment of Saphenous Vein Grafts and Internal Thoracic (Mammary) Arteries
CTA Assessment of Saphenous Vein Grafts and Internal Thoracic (Mammary) Arteries
 Determination of Coronary Calcium
Determination of Coronary Calcium
 Assessment of Left Ventricular Structural Abnormalities
Assessment of Left Ventricular Structural Abnormalities
 Cardiac and Paracardiac Masses
Cardiac and Paracardiac Masses
 Caval Anatomy: Variants and Lesions
Caval Anatomy: Variants and Lesions

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


