, Marilyn J. Siegel2, Tomasz Miszalski-Jamka3, 4 and Robert Pelberg1
(1)
The Christ Hospital Heart and Vascular Center of Greater Cincinnati, The Lindner Center for Research and Education, Cincinnati, OH, USA
(2)
Mallinckrodt Institute of Radiology, Washington University School of Medicine, St. Louis, Missouri, USA
(3)
Department of Clinical Radiology and Imaging Diagnostics, 4th Military Hospital, Wrocław, Poland
(4)
Center for Diagnosis Prevention and Telemedicine, John Paul II Hospital, Kraków, Poland
Abstract
The development of multidetector computed tomography has resulted in marked advancements in the diagnosis of congenital heart disease (CHD) which has renewed interest in the classifications and definitions used to describe the anatomy of the heart and great vessels. The sequential, segmental approach to analyzing CHD patient images was introduced nearly three decades ago and is used worldwide [1–5]. Thus, a thorough understanding of both the nomenclature and anatomy applied in this approach is essential to the proper and error-free interpretation of CHD CTA images [6]. The definitions described below are based on the segmental, sequential approach to classifying CHD which is described in Chap. 5.
The development of multidetector computed tomography has resulted in marked advancements in the diagnosis of congenital heart disease (CHD) which has renewed interest in the classifications and definitions used to describe the anatomy of the heart and great vessels. The sequential, segmental approach to analyzing CHD patient images was introduced nearly three decades ago and is used worldwide [1–5]. Thus, a thorough understanding of both the nomenclature and anatomy applied in this approach is essential to the proper and error-free interpretation of CHD CTA images [6]. The definitions described below are based on the segmental, sequential approach to classifying CHD which is described in Chap. 5.
4.1 Cardiac Orientation
Cardiac orientation or position refers to the relationship or axis of the base to the apex of the heart and may help to predict the presence of CHD. Early in fetal development, normal embryogenesis [situs solitus (normal atrial positions) and D-bulboventricular loop (normal ventricular positions)], results in the apex of the heart being situated in the right hemithorax. At the beginning of the second month, the apex of the heart migrates to the left hemithorax (normal adult position). In situs inversus with an L-loop (atria are reversed and ventricles are reversed), the opposite occurs (the apex of the heart migrates from the left hemithorax to the right hemithorax). Regardless of atrial situs, all D-loops should complete their development with the heart in the left chest (levocardia). On the contrary, all L-loops should end development with the heart in the right chest (dextrocardia). If the cardiac apex fails to shift, it may result in situs solitus with dextrocardia which is termed dextroversion or situs inversus with levocardia called levoversion. Thus, dextrocardia may occur from a D-loop that fails to shift leftward or an L-loop that completes its rightward shift. Mesocardia (midline heart) occurs when the ventricular apex does not complete its shift. Mesocardia may be associated with concordant (D-loop) or discordant (L-loop) ventricles as well as with heterotaxy syndromes.
Of note, positioning of the heart in the right chest with a left-sided cardiac apex can occur when the contents of the left chest force the heart to the right or when the volume of the right lung is reduced (for instance, due to pulmonary hypoplasia or collapse). This type of positioning is more appropriately termed dextroposition since the axis of the heart is usually normal.
To summarize, three different cardiac situs abnormalities are possible: levocardia, dextrocardia, and mesocardia (Fig. 4.1). Levocardia is defined as a normal cardiac position in the left chest with the cardiac base-to-apex axis pointing from upper right to lower left (normal cardiac base-to-apex axis points left to right). Dextrocardia refers to a heart located in the right chest with the base-to-apex axis pointing from the upper left to the lower right. Mesocardia refers to a heart that is usually in the midline with the base-to-apex axis directly from superior to inferior. Situs solitus with dextrocardia is termed dextroversion and situs inversus with levocardia is called levoversion.
Fig. 4.1
A depiction of the three possible cardiac situs abnormalities
4.2 Nomenclature for Thoracic and Visceral Situs
Situs or sidedness refers to the position or arrangement of structures or organs that are not bilaterally symmetric. There are three possible arrangements: normal also known as solitus, inversus (mirror image of normal), and ambiguous (not clearly solitus or inversus). In the ambiguous situation, features of situs solitus and situs inversus are present in the same person. Here the thoracic and abdominal organs cannot be lateralized and have neither the normal nor mirror image arrangement.
4.2.1 Situs Definitions
Thoracic Situs: The situs of the left and right lung is independent of the cardiac or abdominal situs but instead is identified by the anatomy of the respective bronchi, especially the relationship between the bronchi and pulmonary arteries [7]. The right main bronchus takes a more vertical course and branches at an earlier point than the more horizontally oriented left bronchus. See Fig. 4.2.
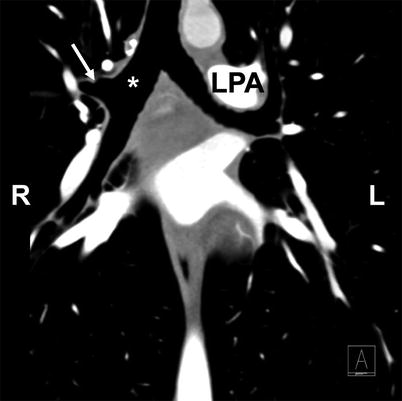
Fig. 4.2
A coronal CT image demonstrating the normal central bronchial anatomy which can be used to help differentiate the morphologic right lung from the morphologic left lung. The right main stem bronchus (asterisk) is more vertically oriented with an early branch point (white arrow), LPA left pulmonary artery
Abdominal Situs: Refers to the sidedness of the main visceral organs such as the liver, stomach, and spleen.
Atriovisceral Situs: Atrial situs is determined by the position of the morphologic right and left atria. Atrial development is simultaneous to venous return formation, and thus, the atrial locations are fixed early in development by the entering veins. The atrial situs is independently determined from and unaffected by the shape of the bulboventricular loop or the final locations of the ventricles. In turn, the atrial situs corresponds to the visceral and thoracic situs and abnormalities in atrial position usually correspond with parallel abnormalities in the visceral and thoracic situs.
Three designations are used in characterizing atrial situs: situs solitus, situs inversus, or situs ambiguous. Situs solitus (normal) and situs inversus are present when there is identifiable lateralization of the atrial chambers, meaning that atrial arrangement is congruent with thoracoabdominal organ arrangement [8, 9]. Situs solitus is present when the right atrium and liver are on the right side and the left atrium, stomach, and spleen are on the left side. The right lung is trilobed and the left lung is bilobed each with their usual bronchial pattern. The right pulmonary artery lies anterior to the right bronchus (eparterial position), and the left bronchus lies behind the left pulmonary artery (hyparterial position). Situs inversus is a mirror image of situs solitus.
It should be noted that atrial situs most often follows the thoracic and visceral situs. That is, atrial situs inversus is most often concomitant with thoracic and visceral situs inversus.
Ambiguous situs indicates that assignment or position of the right and left atria cannot be determined. Ambiguous situs may also be termed heterotaxy. Atrial situs ambiguity usually occurs concomitantly with visceral heterotaxia or situs ambiguity where the visceral organs are abnormally positioned across the left–right axis of the body. The term “isomerism” has been used to describe the combination of atrial situs ambiguity (heterotaxy) and visceral heterotaxy [8, 9]. Two forms of isomerism are recognized: right isomerism and left isomerism. Right isomerism is when there are bilateral morphologic right atria and is associated with asplenia and left isomerism (bilateral morphologic left atria) is associated with polysplenia. Right isomerism is also often associated with bilateral trilobed lungs (two right lungs, a symmetric liver across the midline, and total anomalous pulmonary venous return). Left isomerism is usually associated with bilateral bilobed lungs (two left lungs), interrupted inferior vena cava, and partial anomalous pulmonary venous return.
Note that the aorta and great veins generally have specific orientations depending on the situs and type of isomerism discussed in detail in Chap. 5. See Fig. 5.3.
See Table 4.1 for a characterization of isomerization.
Table 4.1
The characteristics of left and right isomerism
Right isomerism | Left isomerism |
|---|---|
Bilateral morphologic right atria | Bilateral morphologic left atria |
Asplenia | Bilateral bilobed lungs |
Bilateral trilobed lungs | Interrupted inferior vena cava |
Symmetric liver | Partial anomalous pulmonary venous return |
Total anomalous pulmonary venous return |
Figure 4.3 illustrates the thoracic, atrial, and visceral situs seen with situs solitus, situs inversus, and situs ambiguous (right and left isomerism).
Fig. 4.3




Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
