N
%
Patients
24
100
Age (years)
62 ± 11
Females
3
12,5
Diabetes
19
79
Duration of diabetes (years)
19 ± 7
ESRD
20
83
Haemodialysis
17
71
Peritoneal dialysis
3
12,5
Duration of dialysis (years)
4,8 ± 3,9
Diabetes + ESRD
17
71
Connective tissue disorders
2
8
Coronary heart disease
16
66
Cerebrovascular disease
6
25
Inferior limb ischemia
Previous below the ankle amputation
Previous above the ankle amputation
20
8
11
83
33
46
1 Anatomy
BTE vessels include the radial, ulnar, interosseous, and hand arteries (arches, metacarpal, and digital arteries). The most common anatomical variations are the accessory brachial artery and the high origin of radial, ulnar, or interosseous arteries, also known as brachioradial, brachioulnar, or brachioulnoradial arteries. Variations in the distal distribution of the radial and ulnar arteries are common (Fig. 13.1); in normal subjects there is always a significant anastomosis between the radial and the ulnar artery in the hand.
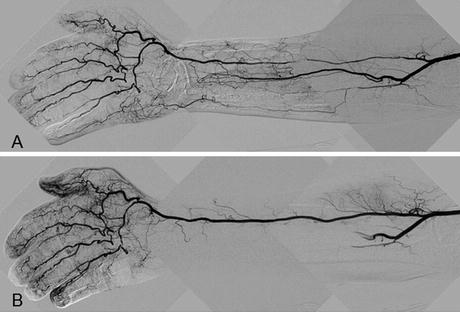
Fig. 13.1
67 years old male type 2 diabetes, ESRD in hemodialysis. Presentation: 4th finger apical gangrene. Retrograde femoral approach. (a) Basal ulnar artery occlusion, dominant radial artery giving both palmar arches presenting diffuse disease of the mid and proximal segment. (b) Final result
2 Disease Definition and Distribution
Table 13.2 shows the data of our CHI patients (24 patients, 30 hands) with pure BTE vessels disease. In each patient it is essential to clarify the causes of the impaired blood flow to the distal tissues, giving to each one the right weight.
Table 13.2
Vascular data of 30 ischemic hands
N | % | |
|---|---|---|
Finger gangrene or ulcer | 30 | 100 |
Radial artery disease | 28 | 93 |
Ulnar artery disease | 29 | 97 |
Interosseous artery disease | 0 | 0 |
Ipsilateral closed AVF | 7 | 23 |
Ipsilateral functioning AVF | 2 | 7 |
(a)
Ulnar and Radial Arteries Occlusive Disease: In the majority of the cases both arteries are affected. These arteries and their distal arches have the same size of coronary and tibial arteries leading to the possibility to treat them with PTA. Interosseous artery was always patent, but its wrist collaterals were insufficient to supply adequate blood flow to the distal bed.
(b)
Small Hand Vessels Occlusive Disease: The extension of occlusive disease to metacarpal and digital arteries plays a major role in generating CHI. Due to their small diameter (<1.5 mm) these vessels are nowadays not amenable to percutaneous treatment.
(c)
Arteriovenous Fistula (AVF): In patients with end stage renal disease (ESRD) in hemodialysis with a functional ipsilateral arteriovenous fistula (AVF) the possibility of a steal syndrome must be considered. A successful PTA of the non-AVF related BTE artery can relief the ischemia saving the AVF for hemodialysis. In case of PTA failure or persistent CHI despite successful BTE vessels PTA, AVF reduction with banding or by a DRIL procedure or if all else fails with closure is mandatory.
3 Disease Distribution
The true incidence is unknown. However it is seen most frequently in patients with coexisting diabetes and end stage renal disease (Table 13.1)
4 Diagnosis: Clinical and Laboratory
BTE arteries occlusive disease presents with symptoms related to chronic CHI: pain at rest and tissue loss. On palpation of the radial and ulnar pulses, one finds the presence of diminished or absent flow. The laboratory abnormalities are those related to ESRD, diabetes, or connective tissue disorders.
5 Diagnostic Imaging: USG/CT/MRI/Diagnostic Angiography
Ultrasound is the cornerstone of noninvasive evaluation of the BTE arteries. It provides quantitative and qualitative information and locates stenosis and occlusions. All major arteries of the upper extremity are identified, including the digital vessels.
CT scan or MR angiography are generally not as helpful, given the reduced sensitivity of these modalities for small vessel occlusive disease..
Diagnostic angiography is essential in confirmation of the diagnosis and treatment choice. It can be performed either via retrograde femoral or antegrade brachial approach (see below, VIII). We generally perform in one step diagnostic angiography and PTA. Multiple views, subtraction techniques, and magnification should be utilized to provide necessary details.
In the presence of an active AVF, before contrast dye injection, inflate a sphygmomanometer at the arm level at a pressure similar to patient systolic blood pressure.
6 Management
Currently, only symptomatic CHI patients should be treated. Data for asymptomatic cohort is missing.
7 List of the Open Operative Choices
1.
Thoracoscopic sympathectomy
2.
Autogenous vein bypass grafting