BENIGN AND MALIGNANT MENINGEAL TUMORS
KEY POINTS
- Extracranial meningiomas are rare and in reality usually turn out to be transcranial extensions of intracranial tumors.
- When a transcranial tumor is present, a meningioma should always be considered in the differential diagnosis.
- The intraosseous component of a meningioma may not be obvious.
- Entire intraosseous meningioma enters the differential diagnosis of intraosseous lesions, especially of the central skull base and petrous apex region.
CLINICAL PERSPECTIVE AND PATHOLOGY
Meningiomas are almost always benign and intracranial; the most common ones originate along the cerebral convexities (Fig. 31.1). They arise from meningothelial arachnoidal cells. Meningiomas usually occur in women.1 They are very common intracranial neoplasms and are most often discovered in middle age. Meningiomas arising entirely outside of the neural axis are rare.
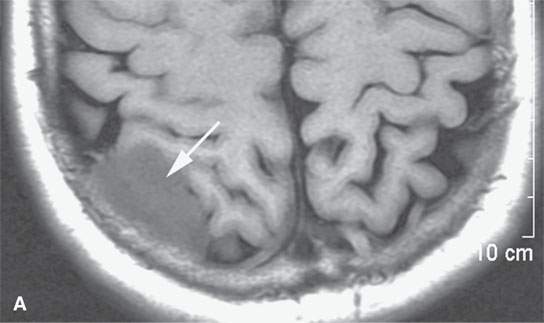
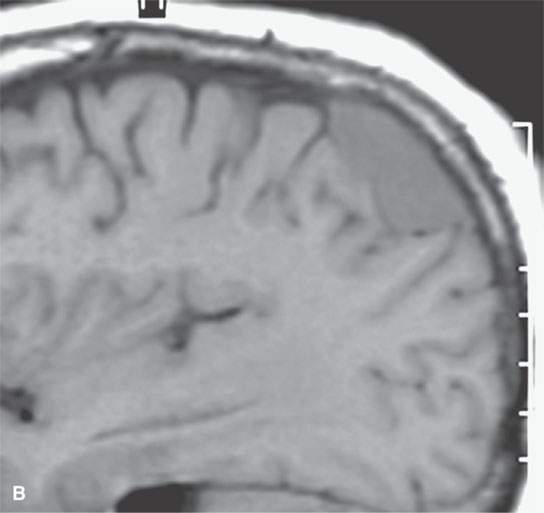
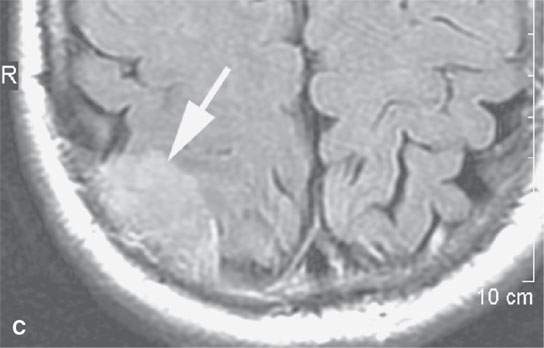
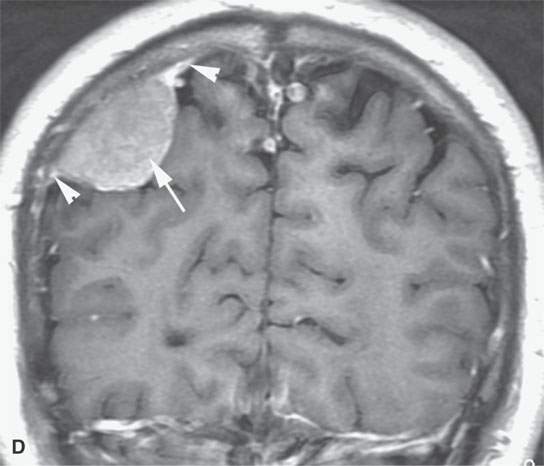
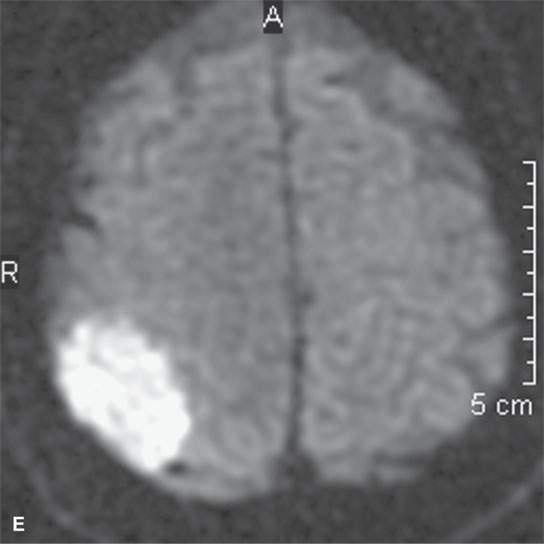
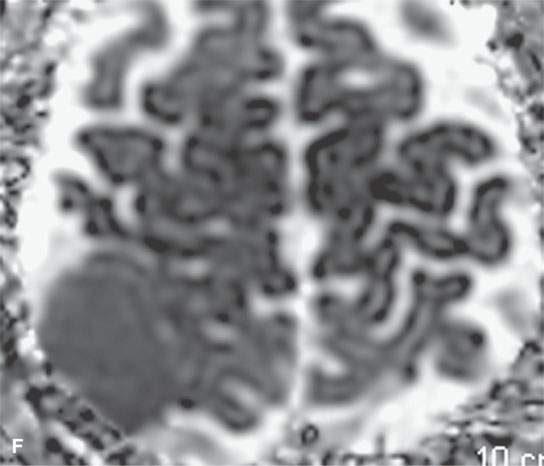
FIGURE 31.1. Magnetic resonance imaging examination of a patient with a convexity meningioma. A: Non–contrast-enhanced T1-weighted (T1W) image showing a likely extra-axial lesion (arrow). B: Sagittal non-contrast-enhanced T1W image confirms extra-axial position of mass. Sometimes, multiplanar viewing is necessary to determine whether a meningioma is intra- or extra-axial. C, D: Axial and coronal contrast-enhanced T1W images showing a fairly typical enhancement pattern of the meningioma (arrows) and typical interface with dura and a small amount of dural enhancement beyond the main mass (arrowheads). E: Diffusion-weighted image shows this highly cellular tumor to demonstrate restricted diffusion—a finding confirmed in the apparent diffusion coefficient (ADC) map in (F).
True extracranial meningiomas can occur in the calvarium, scalp, orbit, nose, paranasal sinuses (Fig. 31.2), middle ear, and infratemporal fossa.1–4 Lesions of the cheek, neck, and parotid have also been reported. Most extracranial meningiomas are simply extracranial extensions of transcranial meningiomas or those arising from the skull base (Figs. 31.3–31.6). Others arise from meningeal extensions along nerve sheaths such as the optic sheath meningioma (Figs. 31.7–31.11), and some are rare metastases from malignant intracranial lesions.5–7
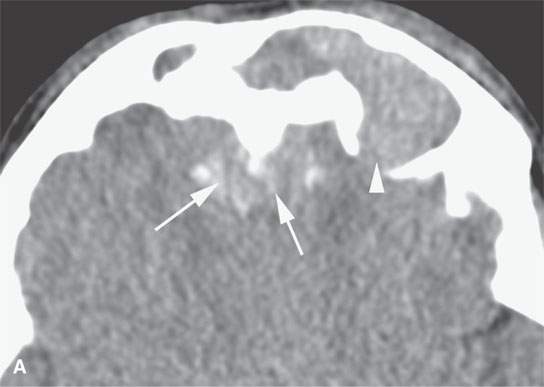

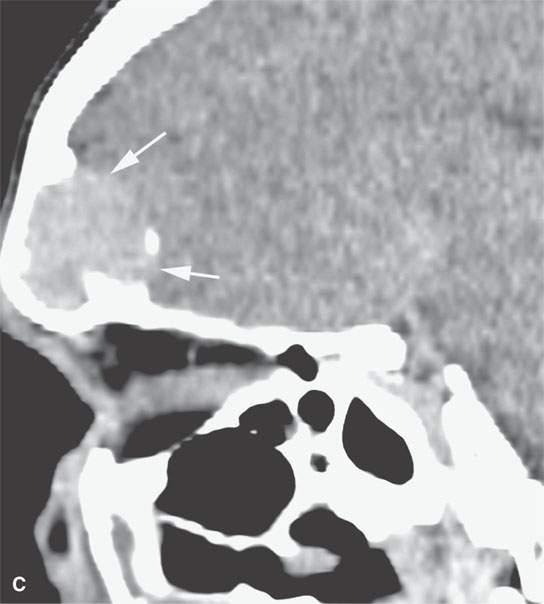
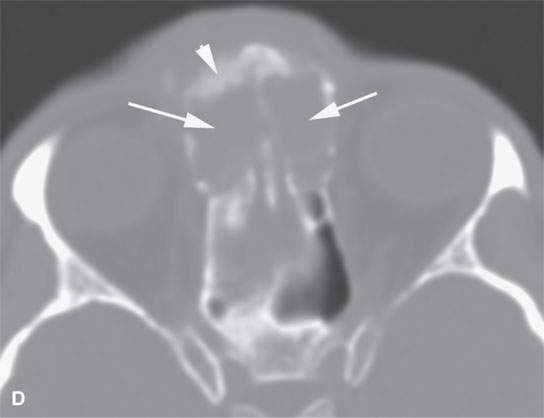
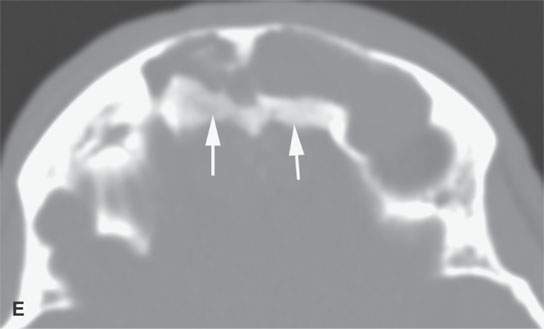
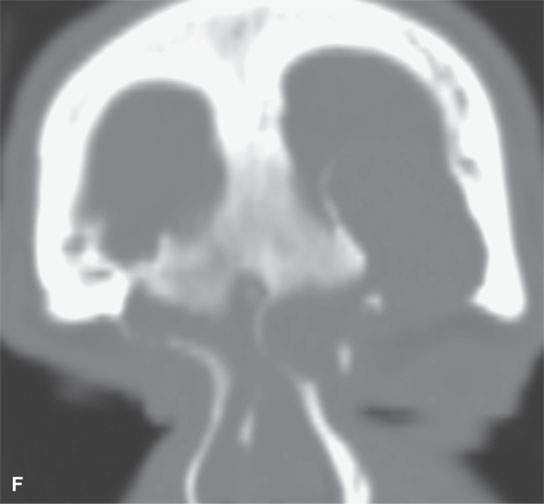
FIGURE 31.2. Contrast-enhanced computed tomography of a meningioma arising within the frontal sinus. A: The axial section shows the mass to be centered in the frontal sinus bowing the inner table inward toward the brain (arrowhead) with only a relatively small component of the tumor spreading along the dura intracranially from the sinus (arrows). B: Sagittal image shows a relatively small component of tumor intracranially (arrows) while tumor fills the region of the frontal recess (white arrowhead) and the frontal sinus (black arrowhead). C: Sagittal image shows the meningioma expanding the sinus and bulging intracranially (arrows)—another sign that localizes this to being a primarily extracranial-origin meningioma arising within the frontal sinus. D: Bone windows show the reactive bone fairly typical of meningioma and the expansion of the sinuses as well as the component of the mass within the frontal recess and anterior ethmoid region (arrows). E: Axial bone windows somewhat higher than the image in (D) shows reactive bone involving the inner table as seen in the coronal image in (F).
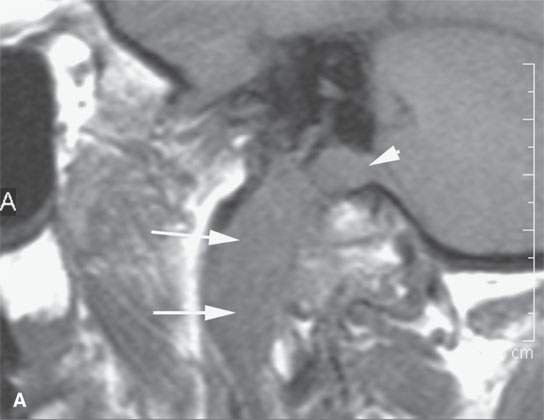

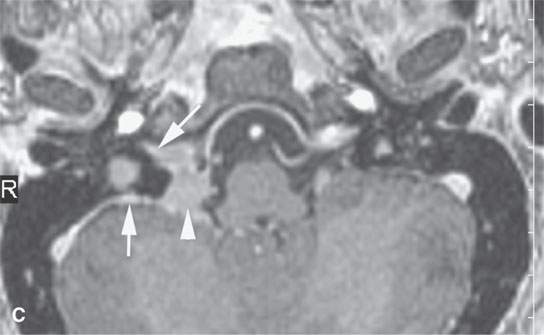
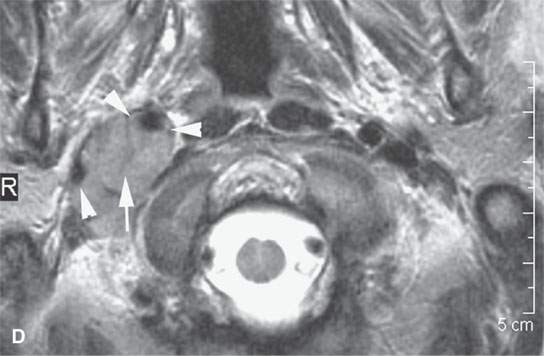
FIGURE 31.3. Contrast-enhanced magnetic resonance study of a patient with a transcranial meningioma arising in the jugular fossa. A: Non–contrast-enhanced T1-weighted (T1W) image shows the extracranial portion of the tumor extending along the carotid sheath (arrows) and the component within the jugular fossa beginning to extend intracranially (arrowhead). B: Oblique reformation of a contrast-enhanced T1W image showing the homogeneously enhancing extracranial (arrows) and intracranial (arrowhead) extension of the tumor. C: Contrast-enhanced T1W image showing intracranial, intradural extension of the tumor (arrowhead) with components extending from the jugular fossa to the dura along the anterior wall of the posterior cranial fossa (arrows); the more linear area of dural involvement could be reactive or actual tumor. D: The extracranial component of the tumor extends along the carotid sheath (arrow) to encase the carotid artery and jugular vein (arrowheads). Note that on this T2-weighted (T2W) image, the mass is equivalent to the brain stem in signal intensity. Most meningiomas on T2W images approach the signal intensity of gray and or white matter.


FIGURE 31.4. Magnetic resonance and computed tomography (CT) images of a transcranial meningioma arising at the foramen ovale region. A: Contrast-enhanced T1-weighted image shows the enhancing transcranial mass with an appearance fairly typical of meningioma. Note the remodeling of the skull base (arrows). B: On this coronal CT study with bone windows, the nature of the skull base remodeling is better depicted as likely chronic and partially reactive (arrowheads) compared to the normal foramen ovale (arrow).
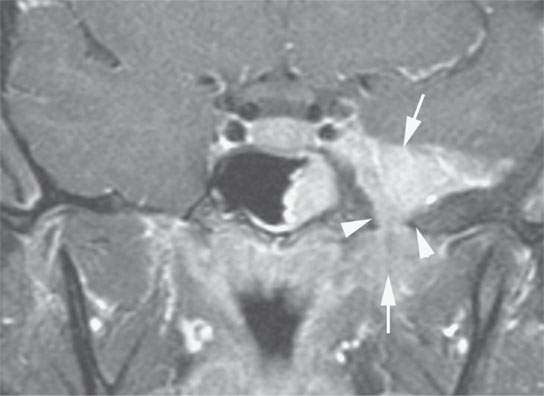
FIGURE 31.5. Contrast-enhanced T1-weighted image of a transcranial meningioma arising along the dura of the floor of the middle cranial fossa showing a more diffuse dural mass than in Figure 31.4. The mass likely is arising from the dura of the middle cranial fossa floor. The mass (arrows) extends transcranially through the foramen ovale; the bone in this region shows chronic thickening and smooth remodeling (arrowheads).
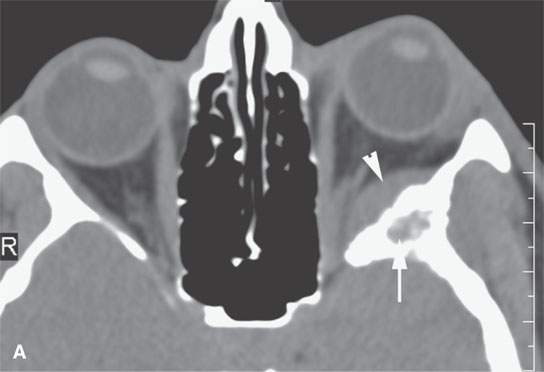
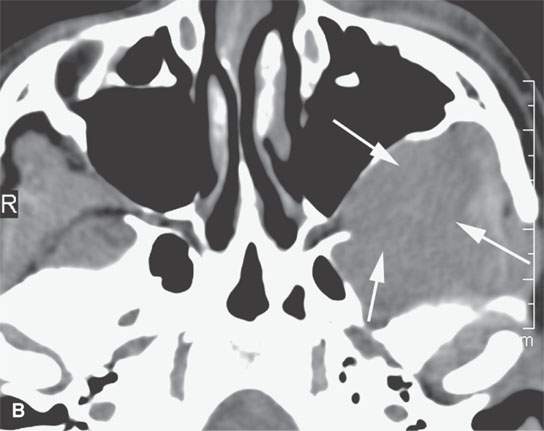
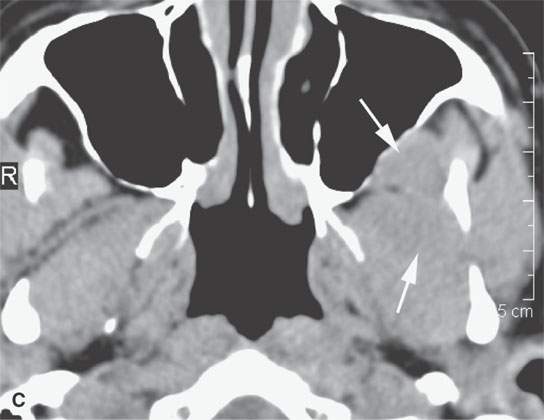
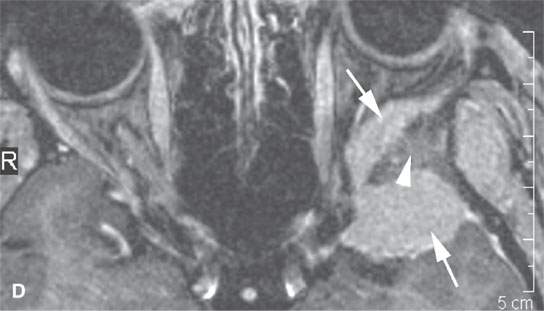
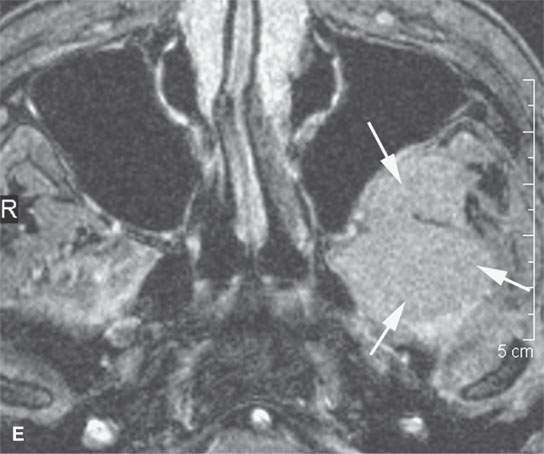
FIGURE 31.6. Computed tomography (CT) and magnetic resonance study of a meningioma presenting as facial pain. A: Non–contrast-enhanced CT showing the extraconal soft tissue mass (arrowhead) and reactive bony changes (arrow) along the greater wing of the sphenoid bone. B: Non–contrast-enhancedCT showing the mass (arrows) to be slightly less dense than muscle, suggesting that it might have atypical features; however, in (C), the mass is about the same density as muscle (arrows). C: Contrast-enhanced T1-weighted (T1W) image shows the intra- and extraosseous component of the mass. The orbital and dural components (arrows) surround the greater wing of the sphenoid, which is infiltrated by meningioma (arrowhead). D, E: Contrast-enhanced T1W image shows the extension into the masticator space and fat pad posterior to the maxillary sinus (arrows). Biopsy revealed an atypical meningioma believed to represent a low-grade malignancy.

FIGURE 31.7. Contrast-enhanced computed tomography (CT) of a patient with optic sheath meningioma. Prior to magnetic resonance imaging, CT was the primary means of diagnosing optic sheath meningiomas. This was frequently accomplished in subtle lesions by recognizing relatively small amounts of thickening or calcification of the optic sheath, as seen in this patient with an optic sheath meningioma on the right (arrow) compared to the normal optic sheath on the left (arrowhead).
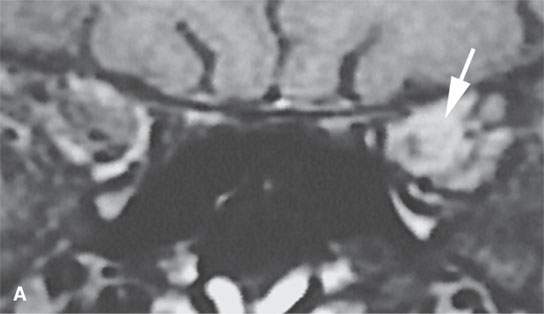
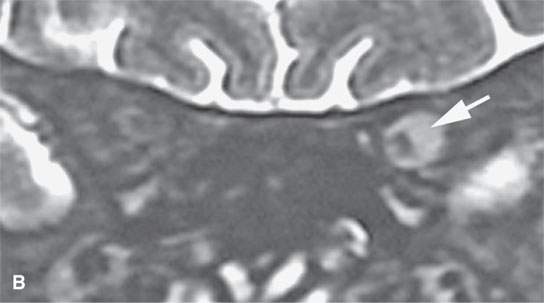
FIGURE 31.8. Magnetic resonance study of a patient with a typical optic sheath meningioma confined to the orbit area. Coronal images are best to evaluate the extent of optic sheath meningioma. A: Coronal T1-weighted image with contrast shows the eccentrically and homogeneously enhancing optic sheath meningioma encasing the optic sheath (arrow) and displacing the optic nerve. B: T2-weighted coronal image shows the meningioma to be hyperintense to the brain and encasing the optic sheath and nerve (arrow).
Related posts:
 Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
 Necrotizing (“Malignant”) Otitis Externa
Necrotizing (“Malignant”) Otitis Externa
 Cervicothoracic Junction: Brachial Plexus Trauma
Cervicothoracic Junction: Brachial Plexus Trauma
 Oropharynx: Introduction
Oropharynx: Introduction
 Branchial Apparatus Developmental Anomalies
Branchial Apparatus Developmental Anomalies
 Mandible and Maxilla: Odontogenic Tumors and Cysts
Mandible and Maxilla: Odontogenic Tumors and Cysts
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


