Benign Causes of FDG Activity
Todd M. Blodgett, MD
Alex Ryan, MD
Key Facts
Terminology
Nonmalignant areas of increased metabolism
Benign nonphysiologic uptake of FDG may be encountered in as many as 25% of studies
As many as 75% of those lesions will be inflammatory
Imaging Findings
Similar imaging findings may be present for malignant and various benign processes
History is critical for reducing misinterpretation
FDG activity in a typical distribution suggests a benign process
Sarcoidosis, fungal infections, post-radiation, postsurgical, and other benign processes may have recognizable patterns of involvement
Top Differential Diagnoses
Malignancy
Benign Masses
Iatrogenic
Inflammation
Infection
Granulomatous Disease
Pathology
Activated inflammatory cells have greatly elevated levels of glycolysis
Diagnostic Checklist
Accurate differentiation between malignant and benign disease can reduce unnecessary surgical explorations
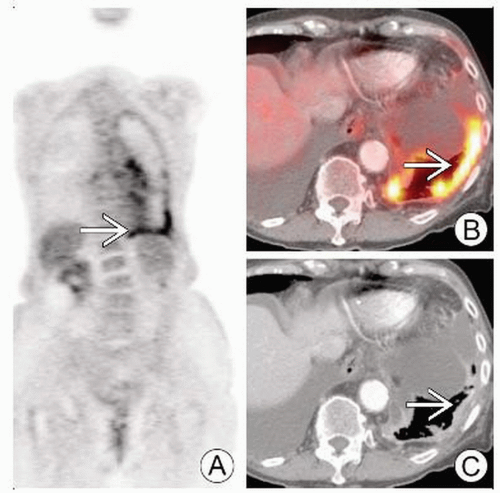 Multiple images (A, B, C) show inflammation  from talc pleurodesis. PET may be positive indefinitely. from talc pleurodesis. PET may be positive indefinitely. |
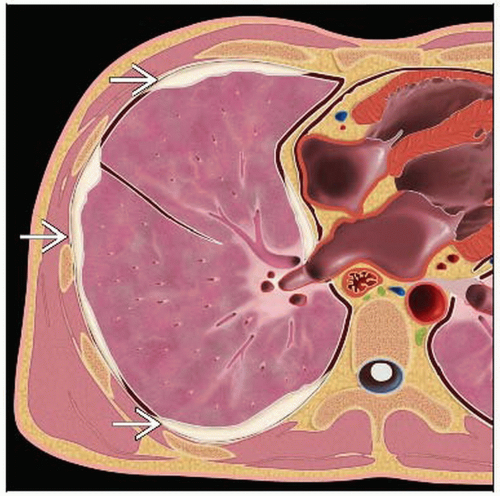 Graphic shows a representation of talc pleurodesis  . The talc is often discontinuous. . The talc is often discontinuous. |
TERMINOLOGY
Abbreviations and Synonyms
Nonmalignant areas of increased metabolism
Definitions
Benign nonphysiologic uptake of FDG may be encountered in as many as 25% of studies
As many as 75% of those lesions will be inflammatory
IMAGING FINDINGS
General Features
Best diagnostic clue
FDG activity in a typical distribution suggests a benign process
Sarcoidosis, fungal infections, post-radiation, postsurgical and other benign processes may have recognizable patterns of involvement
Location: Varies
Nuclear Medicine Findings
Tuberculoma and tuberculous lymphadenopathy
Tuberculoma well-known cause of intense FDG uptake
Appears as discrete nodule or mass with central caseous necrosis and surrounding inflammatory mantle
Sarcoidosis
Typical distribution is bilateral hilar and right paratracheal
FDG uptake secondary to accumulation of Tlymphocytes and mononuclear phagocytes and noncaseating epithelioid granulomas
Intensity of FDG uptake may reflect activity of disease
Multisystem disease
Easily misinterpreted as malignancy
Thus FDG PET most useful for response to treatment and evaluation of extent of disease
Cryptococcosis
Caused by Cryptococcus neoformans
Infection occurs by inhaling fungus into lung
Lung lesions generally demonstrate intense granulomatous inflammation
Several reports have shown false positives due to high FDG uptake
Paragonimiasis
Endemic to southern Asia
Parasitic disease with larval damage ultimately in lungs and brain
Reported cause of high FDG uptake
Abscesses
Glycolytic metabolism elevated in association with leukocytic infiltration
Usually has central photopenia secondary to necrosis or pus
Pneumocystis
Associated with high FDG uptake
Other infections
Sinusitis, pneumonia, radiation-induced pneumonitis, pancreatitis
Each may show elevated FDG uptake
Radiation pneumonitis/fibrosis
FDG uptake caused by infiltration of leukocytes and macrophages
Radiation leads to production of local cytokines including IL-6, TNF, and TGF-beta, which provoke inflammatory morphologic changes
Early after radiation to the lung, PET may be positive (up to several months); may not be able to interpret effect on underlying tumor until resolution
Pneumoconiosis
Parenchymal reaction to presence of foreign substances in lungs
May present with massive fibrosis and associated FDG uptake
Peri-tumoral granulation tissue
Granulation tissue surrounding tumor and inflammatory cells within necrotic areas of tumor contribute to FDG uptake in tumors
As much of 24% of concentration may be due to non-tumor tissue
Chemotherapy
FDG uptake generally decreases after chemotherapy, correlating with clinical response
Splenic uptake
In the setting of infection, splenic uptake can be intense
Spleen has multiple roles in the immune response, reflected in increased FDG activity in patients with infection or inflammation
AIDS
This patient group is vulnerable to a wide range of infections and malignancies
Difficult to distinguish infection from tumor
Toxoplasmosis can be differentiated from lymphoma because it is much less FDG avid, with virtually no overlap in SUV
Fever of undetermined origin
Diagnosis entails 3 weeks duration, episodic fever exceeding 38.3° C, and no diagnosis after standard workup
Causes include infection, neoplasms, collagen vascular disease, granulomatous disease, pulmonary emboli, CVA, and drug fever
FDG PET provides helpful information in 41% of cases
Negative FDG PET makes it very unlikely that a morphologic origin of the fever will be identified
In spite of normal cardiac uptake, FDG PET aids in identification of sites of infective endocarditis
Post-operative uptake
Several weeks should elapse prior to imaging to reduce likelihood of positives due to post-operative changes
Good sensitivity for identification of infection in post-operative patients
Wound healing, such as tracheostomy and colostomy sites or indwelling stents, commonly show elevated FDG uptake
Osteomyelitis
Useful for detection of osteomyelitis
Inflammatory arthritis, acute fracture, and normal healing bone may also cause positive signal
Prosthetic joint infection
Commonly seen due to high prevalence of hip and knee arthroplasties
Joint infection vs. aseptic loosening is a difficult differentiation
FDG PET does not effectively distinguish the two conditions, as they are both inflammatory
Bone fractures
Degree of FDG accumulation usually modest in rib fractures, but may closely mimic malignancy
FDG uptake in healing bone can be present as late as 6 months after the injury
Arthritis
FDG uptake seen especially in acromioclavicular, sternoclavicular, and glenohumeral joints
Uptake can be intense and asymmetric, leading to misinterpretation as neoplasm
Spinal osteomyelitis
Usually confined to vertebral body and intervertebral disk
MR is imaging modality of choice for diagnosis
FDG PET has similarly high sensitivity and specificity
Vasculitis
FDG uptake in giant cell arteritis, Takayasu disease, aortitis, and unspecified large vessel vasculitis has been described
Lymph Nodes
Uptake in lymph nodes is not specific for malignant neoplasm
Granulomatous diseases such as tuberculosis and sarcoidosis may provoke intense FDG uptake in lymph nodes
Necrotic lymph nodes may show poor accumulation
DIFFERENTIAL DIAGNOSIS
Malignancy
When in doubt, consider short term follow-up exam to differentiate
Benign Masses
Adenomas can have focal intense FDG activity
Indistinguishable from malignancy
Iatrogenic
History is imperative for reducing misinterpretation
Inflammation
Almost any inflammatory process may cause false positives on FDG PET
Consider dual-phase PET imaging
Infection
Clinical symptoms often helpful for differentiating malignancy from benign process
Granulomatous Disease
Sarcoidosis and other granulomatous processes can often mimic malignancy
Look for other clues such as distribution, calcifications, and lack of features suggesting malignancy
PATHOLOGY
General Features
General path comments
Inflammatory cells such as neutrophils and activated macrophages at site of inflammation or injection show increased FDG accumulation
Active granulomatous disease, other infectious processes, and active fibrosis may also show FDG uptake and cause false positives
Activated inflammatory cells have greatly elevated levels of glycolysis
20-30x increased in hexose monophosphate shunt, which accounts for high FDG uptake
DIAGNOSTIC CHECKLIST
Consider
Accurate differentiation between malignant and benign disease can reduce unnecessary surgical explorations
Dual-phase or delayed-phase PET imaging may be helpful for distinguishing between malignancy and benign processes
Hyperglycemia promotes greater glucose utilization in inflammatory cells
Leads to more false positives in the setting of elevated blood glucose
SELECTED REFERENCES
1. Chryssikos T et al: FDG-PET imaging can diagnose periprosthetic infection of the hip. Clin Orthop Relat Res. 466(6):1338-42, 2008
2. Chundru S et al: Granulomatous disease: is it a nuisance or an asset during PET/computed tomography evaluation of lung cancers? Nucl Med Commun. 29(7):623-7, 2008
3. Nigg AP et al: Tuberculous Spondylitis (Pott’s Disease). Infection. 36(3):293-4, 2008
4. Saleem BR et al: Periaortic endograft infection due to Listeria monocytogenes treated with graft preservation. J Vasc Surg. 47(3):635-7, 2008
5. Balink H et al: Diagnosis of abdominal aortic prosthesis infection with FDG-PET/CT. Vasc Endovascular Surg. 41(5):428-32, 2007
6. Helleman JN et al: Mycotic aneurysm of the descending thoracic aorta. Review and case report. Acta Chir Belg. 107(5):544-7, 2007
7. Inoue K et al: Diagnosing active inflammation in the SAPHO syndrome using 18FDG-PET/CT in suspected metastatic vertebral bone tumors. Ann Nucl Med. 21(8):477-80, 2007
8. Kang K et al: Positron emission tomographic findings in a tuberculous brain abscess. Ann Nucl Med. 21(5):303-6, 2007
9. Maldonado F et al: Focal organizing pneumonia on surgical lung biopsy: causes, clinicoradiologic features, and outcomes. Chest. 132(5):1579-83, 2007
10. Sheehy N et al: Acute varicella infection mimics recurrent Hodgkin’s disease on F-18 FDG PET/CT. Clin Nucl Med. 32(10):820-1, 2007
11. Lustberg MB et al: FDG PET/CT Findings in Acute Adult Mononucleosis Mimicking Malignant Lymphoma. Eur J Haematol. (In Press)
Image Gallery
 DDx: Focal Intense FDG Activity |
 (Left) Axial CECT shows left maxillary sinus mucosal thickening  and a subtle air-fluid level and a subtle air-fluid level  , compatible with acute sinusitis. (Right) Axial fused PET/CT shows mild to moderately increased FDG activity within the left maxillary sinus , compatible with acute sinusitis. (Right) Axial fused PET/CT shows mild to moderately increased FDG activity within the left maxillary sinus  , compatible with sinusitis. Also note physiologic FDG activity within both palatine tonsils , compatible with sinusitis. Also note physiologic FDG activity within both palatine tonsils  . . |
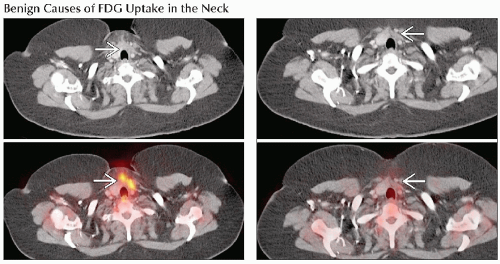 (Left) Axial CECT (top) and PET/CT (bottom) show moderately increased FDG activity  in the thyroidectomy bed in a patient who had a left hemithyroidectomy approximately 3 weeks prior to this scan. (Right) Axial CT (top) and fused PET/CT (bottom), 16 weeks following thyroidectomy, show resolution of the inflammatory activity in the thyroidectomy bed in the thyroidectomy bed in a patient who had a left hemithyroidectomy approximately 3 weeks prior to this scan. (Right) Axial CT (top) and fused PET/CT (bottom), 16 weeks following thyroidectomy, show resolution of the inflammatory activity in the thyroidectomy bed  . . |
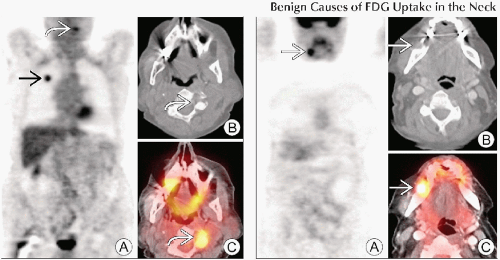 (Left) Coronal PET (A), axial CT (B) and fused PET/CT (C) demonstrate a hypermetabolic right upper lobe mass  , compatible with primary lung cancer, and an incidental focal area of moderately increased FDG activity , compatible with primary lung cancer, and an incidental focal area of moderately increased FDG activity  , corresponding to facet arthrosis in the cervical spine. (Right) Coronal PET (A), axial CT (B) and fused PET/CT (C) demonstrate focally increased FDG activity , corresponding to facet arthrosis in the cervical spine. (Right) Coronal PET (A), axial CT (B) and fused PET/CT (C) demonstrate focally increased FDG activity  in the right maxillary molar, compatible with patient’s history of a dental abscess. in the right maxillary molar, compatible with patient’s history of a dental abscess. |
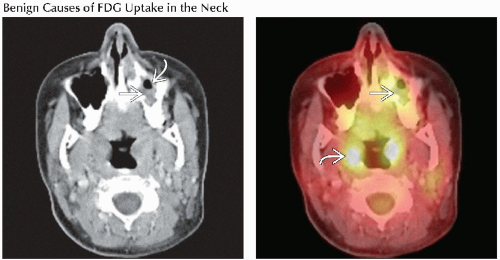
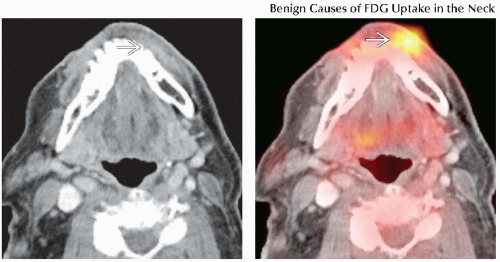 (Left) Axial CECT shows no obvious abnormalities. However, there is some subtle infiltration of the subcutaneous tissues in the anterior jaw  . (Right) Axial fused PET/CT shows a focal area of intense FDG activity . (Right) Axial fused PET/CT shows a focal area of intense FDG activity  in this patient with jaw pain and a history of a dental abscess being treated with antibiotics. in this patient with jaw pain and a history of a dental abscess being treated with antibiotics. |
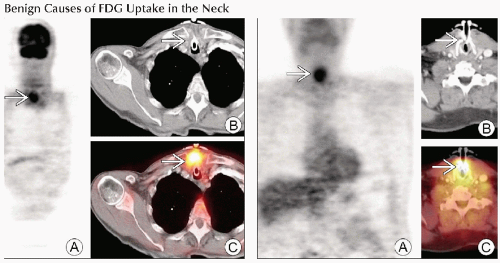 (Left) Approximately 8 weeks after tracheostomy tube placement, coronal PET (A), axial CT (B) and PET/CT (C) demonstrate intense FDG activity surrounding the tube  , compatible with inflammation. (Right) Coronal PET (A), axial CT (B) and PET/CT (C) demonstrate focal intense FDG activity surrounding this patient’s tracheostomy , compatible with inflammation. (Right) Coronal PET (A), axial CT (B) and PET/CT (C) demonstrate focal intense FDG activity surrounding this patient’s tracheostomy  , compatible with inflammation &/or granulation tissue. Almost all tracheostomies will have some degree of increased FDG due to inflammation. , compatible with inflammation &/or granulation tissue. Almost all tracheostomies will have some degree of increased FDG due to inflammation. |
 (Left) Axial CECT shows slight asymmetrical fullness in the left false vocal cord
 . This patient had a history of thyroid carcinoma, status post thyroidectomy, and damage of the left recurrent laryngeal nerve. (Right) Axial fused PET/CT shows focal intense FDG activity in the region of left false vocal cord fullness . This patient had a history of thyroid carcinoma, status post thyroidectomy, and damage of the left recurrent laryngeal nerve. (Right) Axial fused PET/CT shows focal intense FDG activity in the region of left false vocal cord fullness  . Additional history revealed a thyroplasty procedure for paralyzed vocal cord. Teflon may cause a chronic granulomatous reaction, creating intense FDG activity indefinitely. . Additional history revealed a thyroplasty procedure for paralyzed vocal cord. Teflon may cause a chronic granulomatous reaction, creating intense FDG activity indefinitely.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|