In biliary terminology, proximal denotes the portion of the biliary tree closer to liver, whereas distal end denotes the part closer to the bowel.
The right and left hepatic ducts, that is, first-order branches of common hepatic duct (CHD) are routinely visualized on USG.
Normal CHD—5 millimeters.
Normal common bile duct (CBD)—5–6 millimeters. Increase in 1 millimeter per decade noticed after the age of 60, which may increase up to 10–12 millimeters in postcholecystectomy patients.
CBD is visualized as an anechoic duct just above the portal vein at porta hepatis.
Dilated IHBR’s are seen as central and peripheral tubules parallel to portal venules.
Choledocholithiasis (CBD stones)
Primary: De novo formation of stones in the biliary ducts.
Secondary: Migration of stones from GB (or after cholecystectomy).
On USG:
• Echogenic lesions with posterior acoustic shadowing.
• Small stones may lack good acoustic shadows and appear as bright linear echogenicity (Figure 4.1).
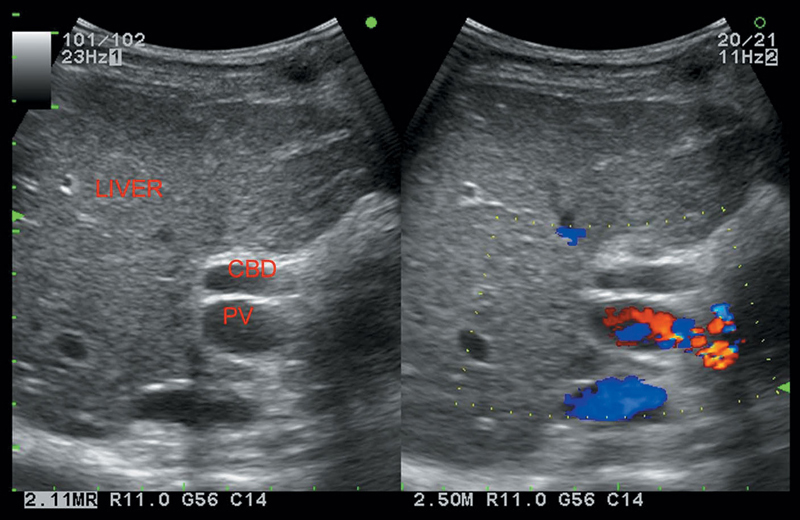
Figure 4.1 Depicting dilatation of CBD.
D/D’s
1. Blood clot (hemobilia), air (pneumobilia), papillary tumors, biliary sludge.
2. Surgical clips due to previous cholecystectomy—short length, high degree of echogenicity, absence of GB, lack of ductal dilation.
• Stone impacted in the cystic duct with surrounding edema.
• Dilatation of biliary ducts to the level of the common hepatic duct.
USG
• Dilatation of the biliary tree (Figure 4.1).
• Choledocholithiasis and sludge.
• Bile duct wall thickening.
• Hepatic abscesses.
Presents with fever, RUQ pain, and jaundice (Charcot’s triad).
Recurrent pyogenic cholangitis
On USG
• Dilated ducts filled with sludge and stones, confined to one or more segments of the liver. Lateral segment of the left lobe is most often involved.
• Chronic biliary obstruction, stasis, and stone formation lead to recurrent episodes of acute pyogenic cholangitis.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


