Fig. 31.1
(a) T2-weighted sagittal MRI before carbon ion radiotherapy. (b) T2-weighted sagittal MRI 4 years after carbon ion radiotherapy. (c) T1-weighted axial MRI with a contrast medium before carbon ion radiotherapy. (d) T1-weighted axial MRI with a contrast medium 4 years after carbon ion radiotherapy
31.4.3 Spinal and Paraspinal Sarcoma
Treatment of spinal and paraspinal tumors makes the best use of the characteristics of the charged particle beam. The treatment of such tumors is complicated by the proximity of lesions to the spinal cord. The radiation tolerance limit using photon beams to the spinal cord is generally quoted at 40–46 Gy in 20–25 fractions.
A “patch combination technique” is used in patients to optimize the dose distribution within tumors of an irregular volume and lying close to the spinal cord. The target volume is divided into two segments, and each segment is treated by a separate radiation field—an anterior/posterior field and a lateral field. By utilizing the sharp dose falloff after the Bragg peak, the distal edge of one field is matched with the lateral edge of the second field. The combination of the two fields and match lines are utilized on alternating days to smear out the potential dose inhomogeneities where the lateral edge of one portal abuts the distal end of the stopping beam [16, 17]. The dose constraint of the carbon ion beams directed to the cross sections involving the spinal cord is 30 GyE administered in 16 fractions; however, radiation-induced myelopathy was quite rare especially in limited experience of C-ion RT; more accumulation of cases and further analysis are needed in the future. The irradiated dose to the spinal cord should be minimized. In our study, as of 2012, C-ion RT was employed in 100 cases with spinal and paraspinal sarcomas, excluding sacral lesions. The patient age ranged from 12 to 84 years (median, 53 years). In principal, a total dose of 64 GyE in 16 fractions and 70.4 GyE in 16 fractions was applied for spinal and paraspinal sarcomas, respectively. The median follow-up duration was 31 months for all patients. At 5 years, the actuarial overall local control rate and overall survival rates were 75 and 51 %, respectively. Two patients in this series developed grade 3 late reactions of the spinal cord. Matsumoto et al. also reported the impact of C-ion RT for 48 spinal sarcomas [18].
31.4.4 Retroperitoneal Sarcoma
Radiotherapy for soft-tissue sarcomas, including retroperitoneal sarcoma, has played an auxiliary role to surgery [19]. C-ion RT has been used in locally advanced unresectable cases; however, the prevalent anatomical conditions may cause technical difficulties. C-ion RT in patients with tumors abutting the small intestine, kidney, and spinal canal is highly risky. In the case of tumors adjacent to the small intestine, placement of surgical spacers made of sheets with minimal foreign body response and less extensive vascularization before C-ion RT is sometimes adopted. The sheets help to separate the intestine from the irradiation field and ensure an adequate margin.
Between May 1997 and February 2006, 24 patients (17 males and 7 females) with unresectable retroperitoneal sarcomas treated with C-ion RT were analyzed [20]. Patient age ranged from 16 to 77 years (median, 48.4 years). Both patients with primary tumors and recurrent tumors were included. Twelve of the patients had undergone chemotherapy for more than 4 weeks prior to radiotherapy. The total dose delivered in most of the cases was 70.4 GyE in 16 fractions. CTVs ranged from 57 cm3 to 1,194 cm3 (median, 525 cm3). At 2 and 5 years, the actuarial overall survival rates were 75 and 50 %, respectively. At 2 and 5 years, the actuarial local control rates were 77 and 69 %, respectively. Grade 3 toxicity was not observed in any case during the follow-up period.
31.4.5 Extremity Sarcomas
C-ion RT for extremity sarcomas is considered in rare cases, such as for tumors in the thigh extending to the proximal and inguinal areas or when the patient is too old to undergo surgery or has comorbidities. C-ion RT might also be considered for the treatment of soft-tissue sarcoma in very elderly patients, such as those in their 80s. Between April 2000 and May 2010, 17 patients with localized primary sarcoma of the extremities underwent C-ion RT. The median patient age was 53 years. Nine patients had primary disease and eight had recurrent disease. Of the 17 patients, eight refused amputation. Tumors were located in the upper limbs in 4 patients and in the lower limbs in 13. Four patients had bone sarcomas and 13 had soft-tissue sarcomas. In 13 of 17 cases, the prescribed dose was 70.4 GyE administered in 16 fractions over 4 weeks. The median follow-up period was 37 months (range, 11–97 months). The radiological response rate was 65 %, whereas the local control rate at 5 years was 76 %. The overall survival rate at 5 years was 56 %. At the end of the follow-up period, 10 of the 17 patients survived without disease progression. Four patients had local recurrence: one patient survived after repeated C-ion RT and the other three died due to systemic diseases. Distant failure was observed in six patients. One patient with femoral chondrosarcoma had a femoral fracture and underwent surgical fixation for 27 months after C-ion RT. No other severe reactions were observed [21].
31.5 Case Study
Case 1: Sacral Sarcoma
A 67-year-old man presented with lumbar pain. MRI revealed a sacral tumor. Needle biopsy was performed, and the tumor was diagnosed as a chordoma. The tumor was deemed unresectable (Figs. 31.1 and 31.2).
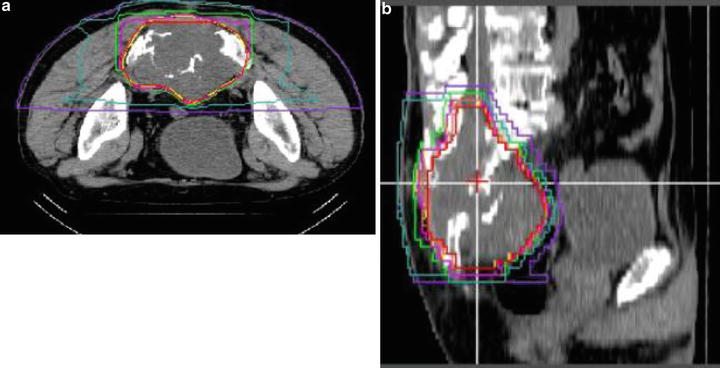
Fig. 31.2
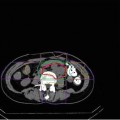
Dose distribution for the patient with sacral chordoma: (a, b) 70.4 GyE in 16 fractions over 4 weeks
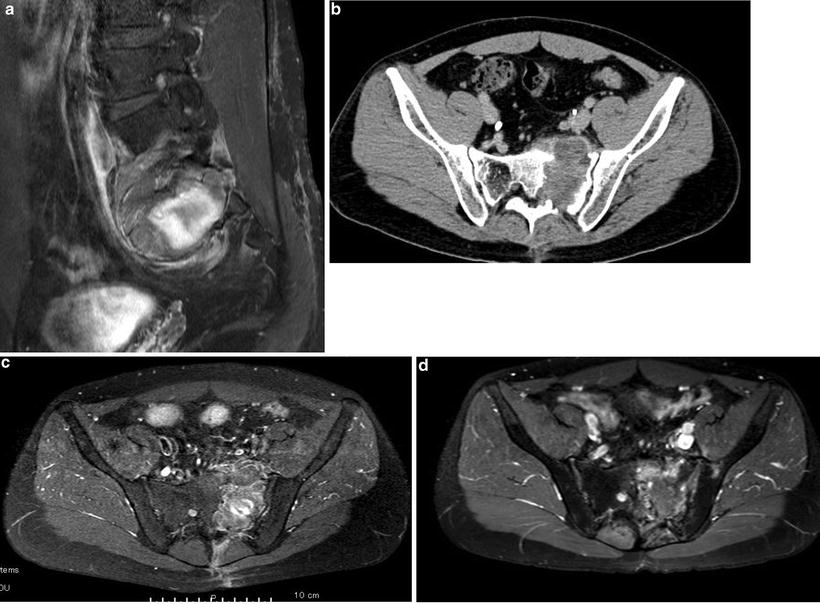
Fig. 31.3
(a) T1-weighted sagittal MRI with a contrast medium before carbon ion radiotherapy. (b) CT image with a contrast medium before carbon ion radiotherapy. (c) T1-weighted axial MRI with a contrast medium before carbon ion radiotherapy. (d) T1-weighted axial MRI with a contrast medium 5 years after carbon ion radiotherapy
Case 2: Sacral Sarcoma
A 25-year-old man presented with left leg pain. A sacral tumor was detected on MRI. Needle biopsy was performed, and the tumor was diagnosed as osteosarcoma. The patient received two cycles of chemotherapy, and the response was no change. The tumor was judged unresectable (Figs. 31.3 and 31.4).
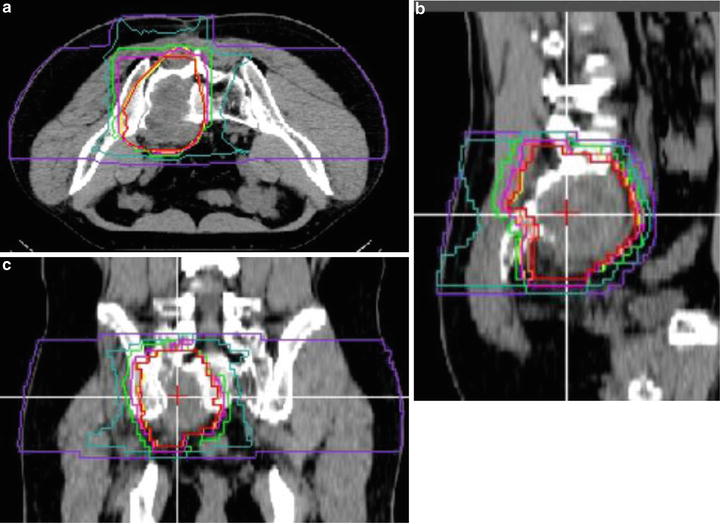
Fig. 31.4
Dose distribution for the patient with sacral osteosarcoma: (a–c) 70.4 GyE in 16 fractions over 4 weeksRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree