Bone Surface Lesion
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Helpful Clues for Common Diagnoses
 Most common bone surface tumor
Most common bone surface tumor
 Metaphyseal or metadiaphyseal in location
Metaphyseal or metadiaphyseal in location
 Majority are solitary
Majority are solitary
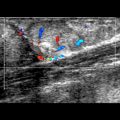
 Variable thickness in hypoechoic cartilage cap
Variable thickness in hypoechoic cartilage cap
 Most osteochondromas are asymptomatic
Most osteochondromas are asymptomatic
 Symptoms can be due to several causes
Symptoms can be due to several causes
 Reactive myositis secondary to friction between osteochondroma and adjacent muscle
Reactive myositis secondary to friction between osteochondroma and adjacent muscle
 Reactive bursitis
Reactive bursitis
 Pseudoaneurysm
Pseudoaneurysm
 Bleeding
Bleeding
 Neurological sequelae
Neurological sequelae
 Fracture
Fracture
 Malignant transformation more common with
Malignant transformation more common with
Helpful Clues for Less Common Diagnoses
 US is very useful at screening for bone tumor recurrence
US is very useful at screening for bone tumor recurrence
 Based on premise that most bone tumor recurrences occur in juxtacortical soft tissues rather than in bone
Based on premise that most bone tumor recurrences occur in juxtacortical soft tissues rather than in bone
 Unlike MR, US assessment of juxtacortical soft tissues is not affected by metallic prosthesis
Unlike MR, US assessment of juxtacortical soft tissues is not affected by metallic prosthesis
 Tumor recurrence usually mirrors imaging characteristics of original tumor
Tumor recurrence usually mirrors imaging characteristics of original tumor
 If recurrence is detected, check regional lymph nodes, as nodal involvement is more frequent with recurrence than with primary bone tumor
If recurrence is detected, check regional lymph nodes, as nodal involvement is more frequent with recurrence than with primary bone tumor ![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Bone Surface Lesion