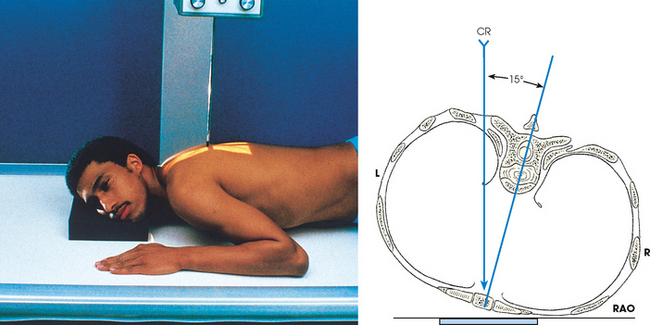
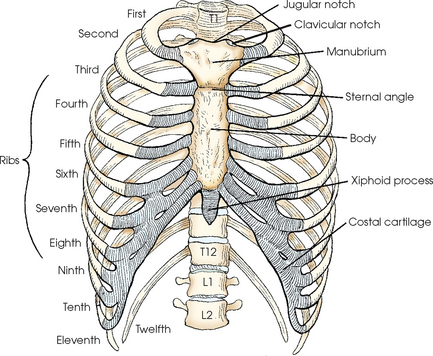
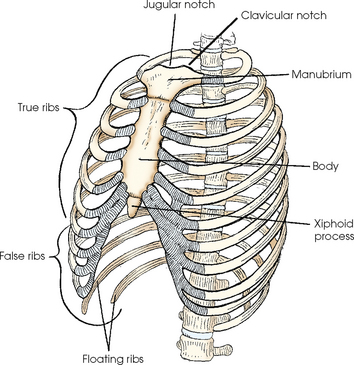
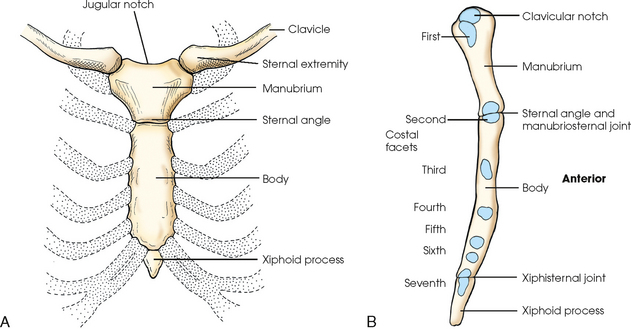
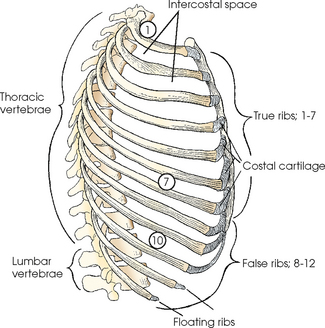
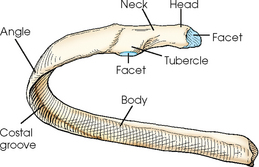
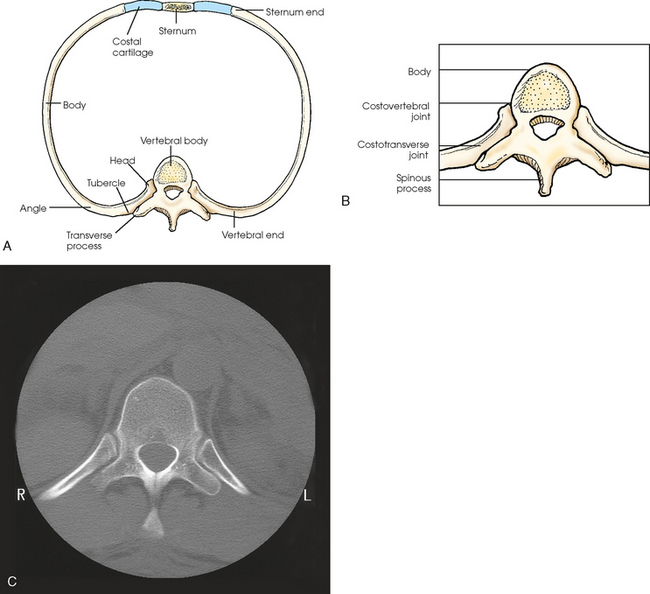
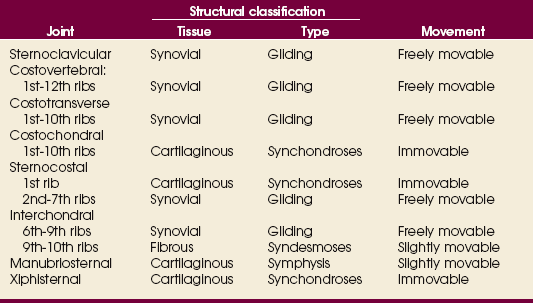
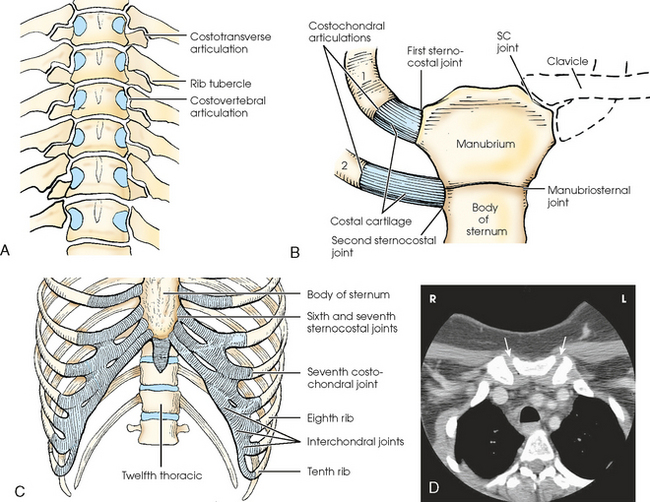
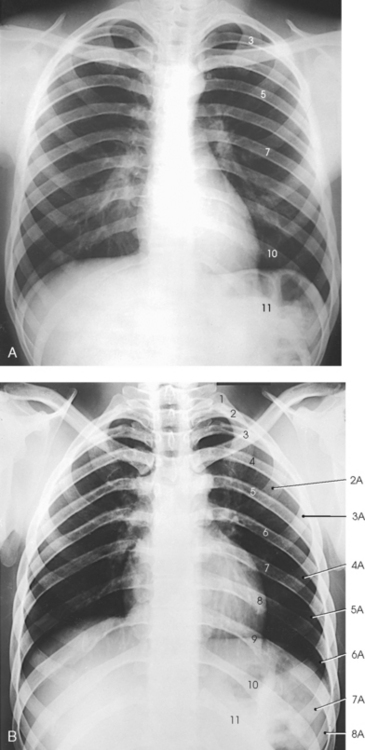
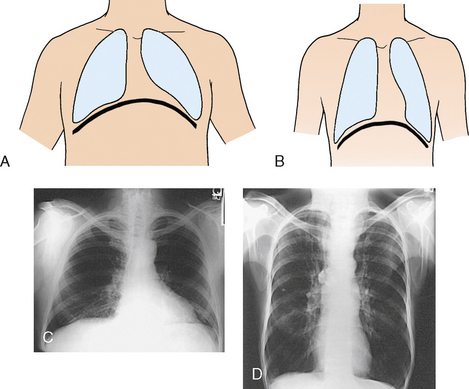
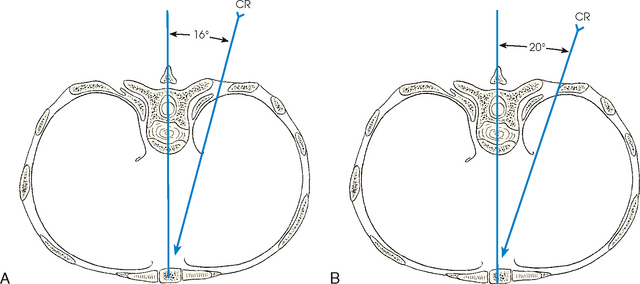
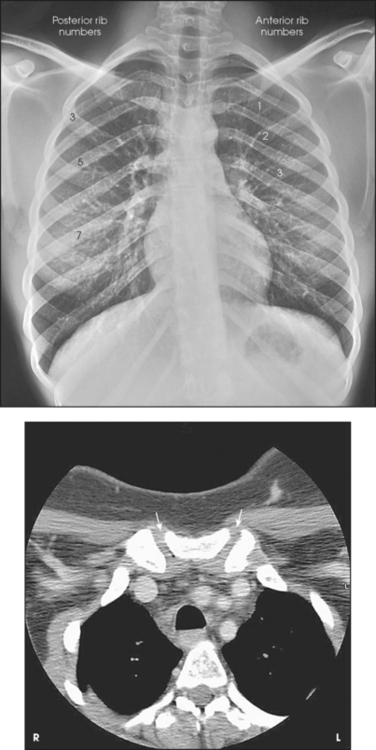
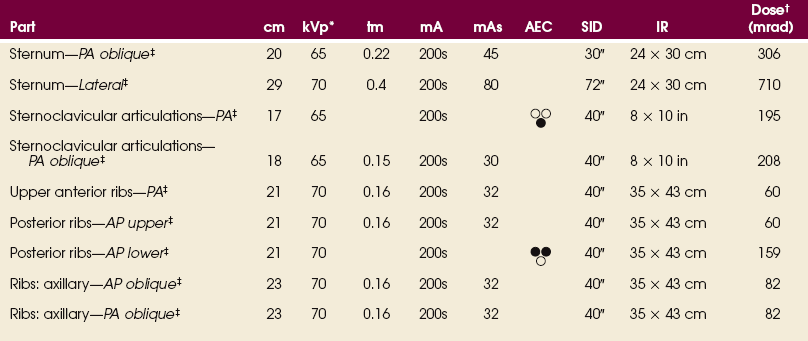
9 The sternum, or breastbone, is directed anteriorly and inferiorly and is centered over the midline of the anterior thorax (Figs. 9-1 to 9-3). A narrow, flat bone about 6 inches (15 cm) in length, the sternum consists of three parts: manubrium, body, and xiphoid process. The sternum supports the clavicles at the superior manubrial angles and provides attachment to the costal cartilages of the first seven pairs of ribs at the lateral borders. The manubrium, the superior portion of the sternum, is quadrilateral in shape and is the widest portion of the sternum. At its center, the superior border of the manubrium has an easily palpable concavity termed the jugular notch. In the upright position, the jugular notch of the average person lies anterior to the interspace between the second and third thoracic vertebrae. The manubrium slants laterally and posteriorly on each side of the jugular notch, and an oval articular facet called the clavicular notch articulates with the sternal extremity of the clavicle. On the lateral borders of the manubrium, immediately below the articular notches for the clavicles, are shallow depressions for the attachment of the cartilages of the first pair of ribs. The 12 pairs of ribs are numbered consecutively from superiorly to inferiorly (Fig. 9-4; see Figs. 9-1 and 9-2). The rib number corresponds to the thoracic vertebra to which it attaches. Each rib is a long, narrow, curved bone with an anteriorly attached piece of hyaline cartilage, the costal cartilage. The costal cartilages of the first through seventh ribs attach directly to the sternum. The costal cartilages of the 8th through 10th ribs attach to the costal cartilage of the 7th rib. The ribs are situated in an oblique plane slanting anteriorly and inferiorly so that their anterior ends lie 3 to 5 inches (7.6 to 12.5 cm) below the level of their vertebral ends. The degree of obliquity gradually increases from the 1st to the 9th rib and then decreases to the 12th rib. The first seven ribs are called true ribs because they attach directly to the sternum. Ribs 8 to 12 are called false ribs because they do not attach directly to the sternum. The last two ribs (11th and 12th ribs) are often called floating ribs because they are attached only to the vertebrae. The spaces between the ribs are referred to as the intercostal spaces. A typical rib consists of a head, a flattened neck, a tubercle, and a body (Figs. 9-5 and 9-6). The ribs have facets on their heads for articulation with the vertebrae. The facet is divided on some ribs into superior and inferior portions for articulation with demifacets on the vertebral bodies. The tubercle also contains a facet for articulation with the transverse process of the vertebra. The 11th and 12th ribs do not have a neck or tubercular facets. The two ends of a rib are termed the vertebral end and the sternal end. The eight joints of the bony thorax are summarized in Table 9-1. A detailed description follows. The sternoclavicular joints are the only points of articulation between the upper limbs and the trunk (see Fig. 9-3). Formed by the articulation between the sternal extremity of the clavicles and the clavicular notches of the manubrium, these synovial gliding joints permit free movement (the gliding of one surface on the other). A circular disk of fibrocartilage is interposed between the articular ends of the bones in each joint, and the joints are enclosed in articular capsules. Posteriorly, the head of a rib is closely bound to the demifacets of two adjacent vertebral bodies to form a synovial gliding articulation called the costovertebral joint (Fig. 9-7, A; see Fig. 9-6). The 1st, 10th, 11th, and 12th ribs each articulate with only one vertebral body. Costochondral articulations are found between the anterior extremities of the ribs and the costal cartilages (see Fig. 9-7, B). These articulations are cartilaginous synchondroses and allow no movement. The articulations between the costal cartilages of the true ribs and the sternum are called sternocostal joints. The first pair of ribs, rigidly attached to the sternum, form the first sternocostal joint. This is a cartilaginous synchondrosis type of joint, which allows no movement. The second through seventh sternocostal joints are considered synovial gliding joints and are freely movable. Interchondral joints are found between the costal cartilages of the sixth and seventh, seventh and eighth, and eighth and ninth ribs (see Fig. 9-7, C). These interchondral joints are synovial gliding articulations. The interchondral articulation between the 9th and 10th ribs is a fibrous syndesmosis and is only slightly movable. The manubriosternal joint is a cartilaginous symphysis joint, and the xiphisternal joints are cartilaginous synchondrosis joints that allow little or no movement (see Figs. 9-3, B, and 9-7, B and C). On deep inspiration, the anterior ends of the ribs are carried anteriorly, superiorly, and laterally while the necks are rotated inferiorly (Fig. 9-8, A). On deep expiration, the anterior ends are carried inferiorly, posteriorly, and medially, while the necks are rotated superiorly (Fig. 9-8, B). The last two pairs of ribs are depressed and held in position by the action of the diaphragm when the anterior ends of the upper ribs are elevated during respiration. The position of the diaphragm varies with body habitus: It is at a higher level in hypersthenic patients and at a lower level in asthenic patients (Fig. 9-9). In sthenic patients of average size and shape, the right side of the diaphragm arches posteriorly from the level of about the 6th or 7th costal cartilage to the level of the 9th or 10th thoracic vertebra when the body is in the upright position. The left side of the diaphragm lies at a slightly lower level. Because of the oblique location of the ribs and the diaphragm, several pairs of ribs appear on radiographs to lie partly above and partly below the diaphragm. *kVp values are for a three-phase, 12-pulse generator or high frequency. †Relative doses for comparison use. All doses are skin entrance for average adult at cm indicated. The position of the sternum with respect to the denser bony and soft tissue thoracic structures makes it a difficult structure to radiograph satisfactorily. Few problems are involved in obtaining a lateral projection, but because of the location of the sternum directly anterior to the thoracic spine, an AP or PA projection provides little useful diagnostic information. To separate the vertebrae and sternum, it is necessary to rotate the body from the prone position or to angle the central ray medially. The exact degree of required angulation depends on the depth of the chest, with deep chests requiring less angulation than shallow chests (Fig. 9-10 and Table 9-2). TABLE 9-2 Sternum: thickness and central ray angulation Angulation of the body or the central ray to project the sternum to the right of the thoracic vertebrae clears the sternum of the vertebrae but superimposes it over the posterior ribs and the lung markings (Fig. 9-11). If the sternum is projected to the left of the thoracic vertebrae, it is also projected over the heart and other mediastinal structures (Fig. 9-12). The super imposition of the homogeneous density of the heart can be used to advantage (compare Figs. 9-11 and 9-12). The pulmonary structures, particularly in elderly persons and heavy smokers, can cast confusing markings over the sternum, unless the motion of shallow breathing is used to eliminate them. If motion is desired, the exposure time should be long enough to cover several phases of shallow respiration (Figs. 9-13 and 9-14). The milliampere (mA) must be relatively low to achieve the desired milliampere-second (mAs). Protection of the patient from unnecessary radiation is a professional responsibility of the radiographer (see Chapter 1 for specific guidelines). In this chapter, the Shield gonads statement indicates that the patient is to be protected from unnecessary radiation by restricting the radiation beam using proper collimation. In addition, the placement of lead shielding between the gonads and the radiation source is appropriate when the clinical objectives of the examination are not compromised. SID: A 30-inch (76-cm) source-to-IR distance (SID) is recommended to blur the posterior ribs. See page 31, Chapter 1, for use of a 30-inch (76-cm) SID. • Adjust the elevation of the left shoulder and hip so that the thorax is rotated just enough to prevent superimposition of the vertebrae and sternum. • Estimate the amount of rotation with sufficient accuracy by placing one hand on the patient’s sternum and the other hand on the thoracic vertebrae to act as guides while adjusting the degree of obliquity. The average rotation is about 15 to 20 degrees (Fig. 9-15). Fig. 9-15 PA oblique sternum, RAO position. Line drawing is an axial view (from feet upward). CR, central ray. • Align the patient’s body so that the long axis of the sternum is centered to the midline of the grid. • Place the top of the IR about 1½ inches (3.8 cm) above the jugular notch. • Respiration: When breathing motion is to be used, instruct the patient to take slow, shallow breaths during the exposure. When a short exposure time is to be used, instruct the patient to suspend breathing at the end of expiration to obtain a more uniform density.
BONY THORAX
Sternum
Ribs
Bony Thorax Articulations
RESPIRATORY MOVEMENT
DIAPHRAGM
SUMMARY OF PATHOLOGY
Condition
Definition
Fracture
Disruption of the continuity of bone
Metastases
Transfer of a cancerous lesion from one area to another
Osteomyelitis
Inflammation of bone owing to a pyogenic infection
Osteopetrosis
Increased density of atypically soft bone
Osteoporosis
Loss of bone density
Paget disease
Thick, soft bone marked by bowing and fractures
Tumor
New tissue growth where cell proliferation is uncontrolled
Chondrosarcoma
Malignant tumor arising from cartilage cells
Multiple myeloma
Malignant neoplasm of plasma cells involving the bone marrow and causing destruction of bone
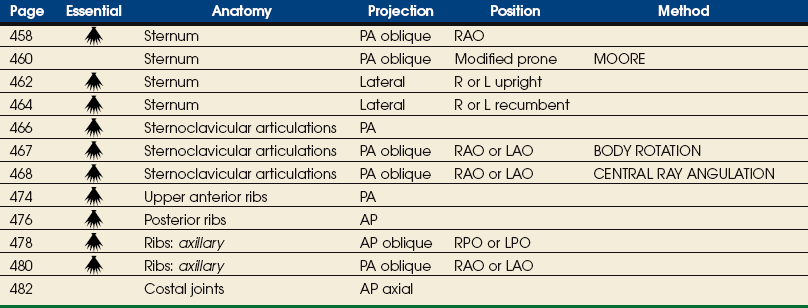
EXPOSURE TECHNIQUE CHART ESSENTIAL PROJECTIONS
Sternum
Depth of thorax (cm)
Depth of tube angulation
15
22
16.5
21
18
20
19.5
19
21
18
22.5
17
24
16
25.5
15
27
14
28.5
13
30
12
Radiation Protection
 PA OBLIQUE PROJECTION
PA OBLIQUE PROJECTION