Presentation and Presenting Images
( ▶ Fig. 15.1, ▶ Fig. 15.2, ▶ Fig. 15.3, ▶ Fig. 15.4)
A 64-year-old female with a distant history of small lymphocytic lymphoma presents for routine screening mammography.
15.2 Key Images
( ▶ Fig. 15.5, ▶ Fig. 15.6, ▶ Fig. 15.7, ▶ Fig. 15.8)
15.2.1 Breast Tissue Density
The breasts are almost entirely fatty.
15.2.2 Imaging Findings
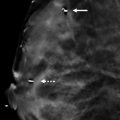
The imaging of the right breast is normal (not shown). The left breast demonstrates a group of calcifications (solid arrow) in the lower inner quadrant at the 7 o’clock location, 12 cm from the nipple. The left breast tomosynthesis localizes the calcifications to the skin and the inferior-most slice, slice 1 of 60 on the left craniocaudal (LCC) tomosynthesis movie ( ▶ Fig. 15.7). A mole on the inferior breast, denoted with a circle skin marker (broken arrow), is also seen on this slice.
15.3 BI-RADS Classification and Action
Category 2: Benign
15.4 Differential Diagnosis
Skin calcifications: The tomosynthesis imaging localizes the calcifications to the inferior-most slice of the CC tomosynthesis movie.
Intraparenchymal calcifications: The calcifications localize to the skin, not within the breast, making this an unlikely possibility.
Artifact: This finding is reproduced on the both conventional and tomosynthesis imaging. It appears to be within the skin and not on the skin, such as many powders or lotions present.
15.5 Essential Facts
Before tomosynthesis was available, tangential films were used to diagnose skin lesions and skin calcifications. Now tomosynthesis imaging can easily and quickly localize findings including calcifications to the dermis.
Skin calcifications may be confused with intraparenchymal calcifications.
Homer and colleagues described the tattoo sign, which can help radiologists differentiate between dermal and intraparenchymal calcifications.
Calcifications that maintain a fixed relationship to each other—the tattoo sign—suggest a dermal location.
Skin calcifications are benign and do not require biopsy.
15.6 Management and Digital Breast Tomosynthesis Principles
If these calcifications were assessed to be suspicious, an attempt at biopsy would have been unsuccessful. Tomosynthesis evaluation would have avoided an unnecessary biopsy.
For the person new to tomosynthesis but with the knowledge that the circular marker denoted a mole on the inferior breast, the location of the mole on slice 1 of 60 on the LCC tomosynthesis movie would have alerted him or her to the dermal location of the calcifications.
Knowing the orientation of the slices makes localizing findings with tomosynthesis easy.
Tomosynthesis can perform all images that conventional mammography can perform, except a magnification view. The inability to perform magnification views is a limitation of tomosynthesis.
15.7 Further Reading
[1] Homer MJ, D’Orsi CJ, Sitzman SB. Dermal calcifications in fixed orientation: the tattoo sign. Radiology. 1994; 192(1): 161‐163 PubMed

Fig. 15.1 Left craniocaudal (LCC) mammogram.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


