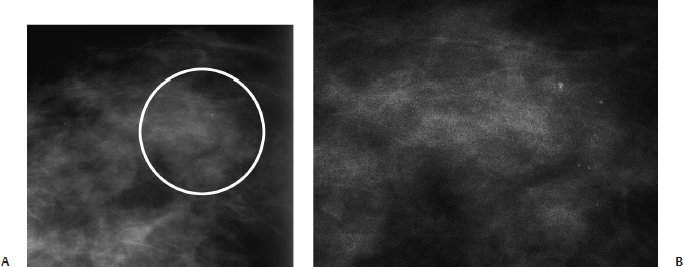
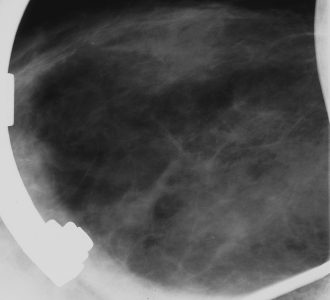
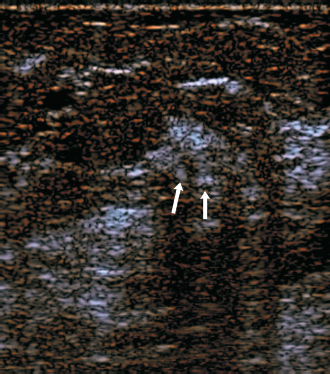
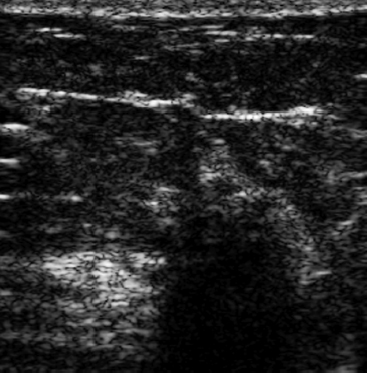
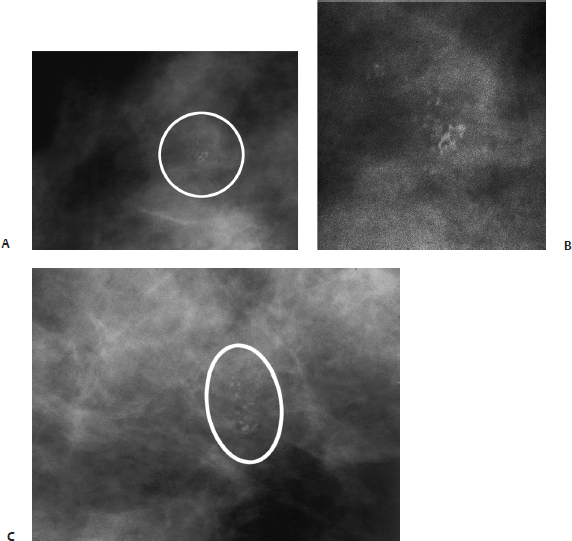
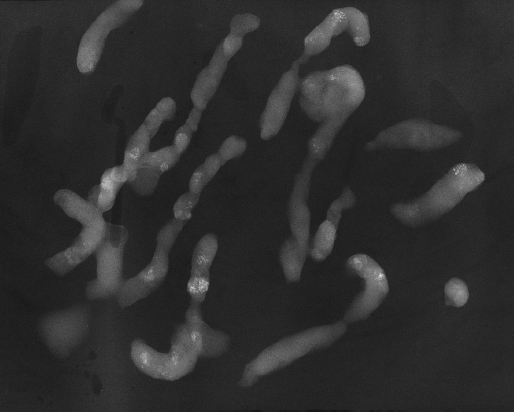
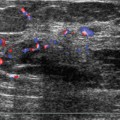
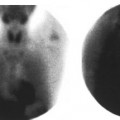
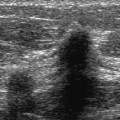
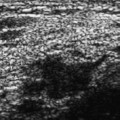
17Calcifications: Amorphous/Indistinct Microcalcifications A 48-year-old woman presents with new densities on her right mammogram. • Normal exam Calcifications (Figs. 17.1 and 17.2) • Type: amorphous/indistinct • Distribution: grouped/clustered Fig 17.1 (A) Right CC mammogram. In the outer breast, multiple amorphous densities were present (circle). These densities could only be identified on this view. (B) Enlargement of circled densities in A. Fig 17.2 Right CC spot magnification mammogram. The patient returned 5 days later, and the densities are no longer present. • Deodorant material on skin • BI-RADS assessment category 2, benign finding • This case is an example of the appearance of skin powder. Various creams, powders, tattoos, and aluminum deodorants can produce densities that may appear to represent intraparenchymal calcifications. When the densities are extremely small and visible on only one view, this etiology should be considered. Bartton JW III, Kornguth PJ. Mammographic deodorant and powder artifact: is there confusion with malignant microcalcifications? Breast Dis 1990;3:121–126 Pamilo M, Soiva M, Suramo I. New artifacts simulating malignant microcalcifications in mammography. Breast Dis 1989;1:321–327 A 64-year-old woman presents with new calcifications on her screening mammogram. • Normal exam Calcifications (Fig. 17.3) • Type: amorphous/indistinct • Distribution: grouped/clustered Fig 17.3 In the upper outer quadrant of the right breast, there is a cluster of indistinct amorphous calcifications (circle). (A) Right MLO magnification mammogram. (B) Enlargement of circled calcifications in A. (C) Right CC magnification mammogram. Low Frequency Frequency • 7 MHz (Fig. 17.4) Fig 17.4 Right radial low-frequency breast sonogram. The calcifications (arrows) identified in Fig. 17.3 were localized sonographically. Lower-frequency sonography is generally more helpful when the breast tissue is extremely attenuating. In this case of fibroadenomatous hyperplasia, the lower frequency demonstrates that there is no mass in the area of the calcifications. Only benign-appearing hyperechoic tissue is present. Frequency • 10 MHz Fig 17.5 Right radial high-frequency breast sonogram. When using the higher frequency, the area of calcification heavily shadows due to the highly attenuating fibrous tissue. The shadowing prevents one from differentiating attenuating benign tissue from malignant tissue. • Fibroadenomatoid hyperplasia • BI-RADS assessment category 4, suspicious abnormality; biopsy should be considered. • These amorphous calcifications are moderately suspicious. Conditions that may produce these calcifications include fibrocystic changes, fibroadenomas, fat necrosis, and intraductal carcinoma. • Fibrosis highly attenuates sound and commonly produces focal shadowing. To differentiate diffuse fibrosis from a focal malignant mass, one should utilize a lower frequency. A lower frequency may penetrate the tissue and demonstrate either the presence of a mass or the presence of benign tissue. Kamal M, Evans AJ, Denley H, Pinder SE, Ellis IO. Fibroadenomatoid hyperplasia: a cause of suspicious microcalcification on mammographic screening. AJR Am J Roentgenol 1998;171:1331–1334 A 49-year-old woman presents with left breast calcifications that are new since her previous screening mammogram 4 years ago. • Normal exam Calcifications (Figs. 17.6 and 17.7) • Type: amorphous/indistinct • Distribution: segmental Fig 17.6 Amorphous calcifications are present throughout the entire left upper outer quadrant. (A) Left MLO mammogram. (B) Left CC mammogram. (C) Left LM magnification mammogram. (D) Enlargement of calcifications in C. Fig 17.7 Specimen radiograph from percutaneous mammographically guided stereotactic core biopsy. Most of the cores exhibit amorphous calcifications. Atypical ductal hyperplasia; both the percutaneous core biopsy and the partial mastectomy specimens demonstrated atypical duct epithelial hyperplasia without evidence of in situ or invasive carcinoma. • BI-RADS assessment category 4, suspicious; biopsy should be considered. • Atypical ductal hyperplasia (ADH) is commonly associated with biopsied calcifications. If the sampled tissue only demonstrates ADH, reexcision of the tissue is recommended. About 50% of percutaneous biopsies showing only ADH are associated with malignancy after subsequent surgical excision. Larger tissue core sampling devices appear to reduce the chance of inadequate sampling to 10 to 20%.
Case 17.1: Skin Powder/Deodorant
Case History
Physical Examination
Mammogram
Pathology
Management
Pearls and Pitfalls
Suggested Reading
Case 17.2: Fibrocystic Change
Case History
Physical Examination
Mammogram
Ultrasound
Pathology
Management
Pearls and Pitfalls
Suggested Reading
Case 17.3: Fibrocystic Change
Case History
Physical Examination
Mammogram
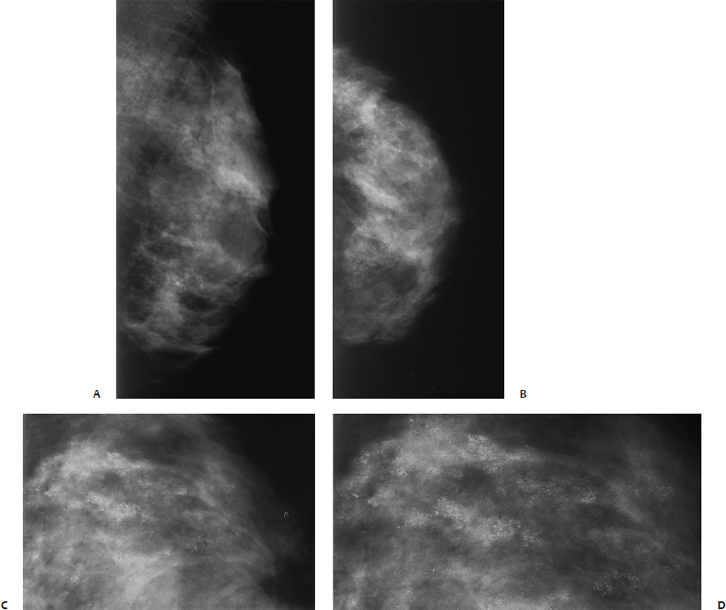
Pathology
Management
Pearls and Pitfalls
Suggested Reading
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


