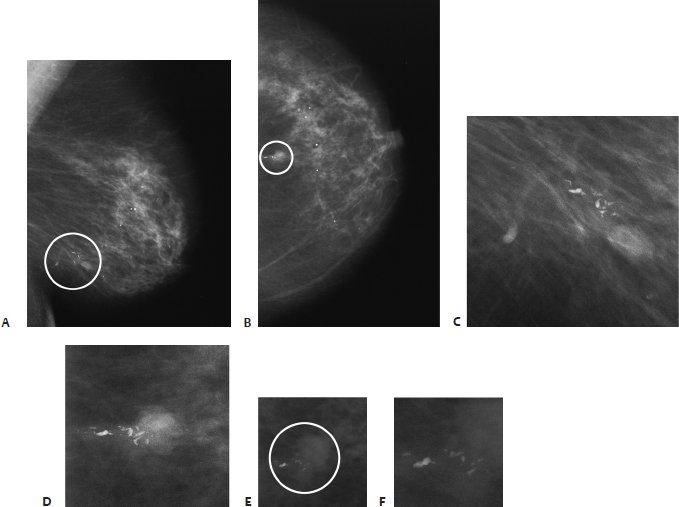
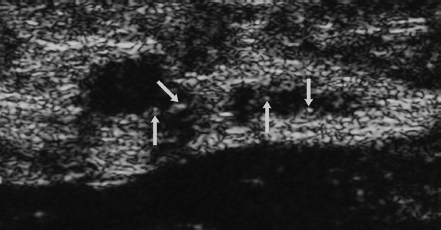
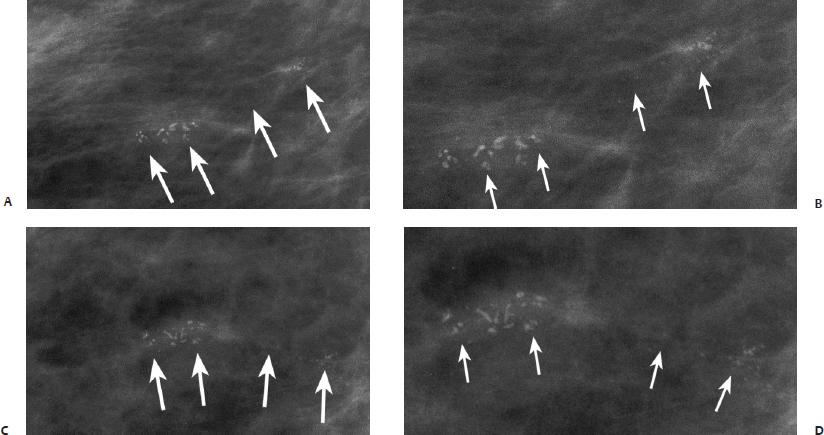
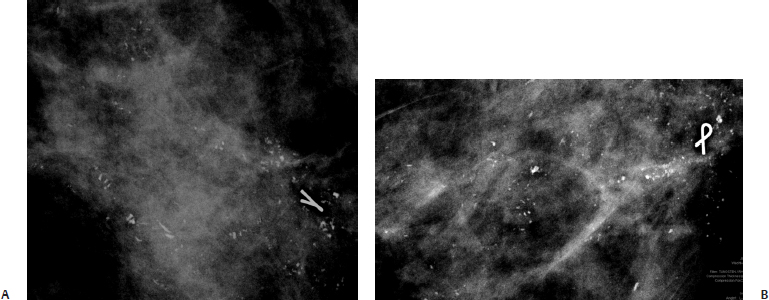
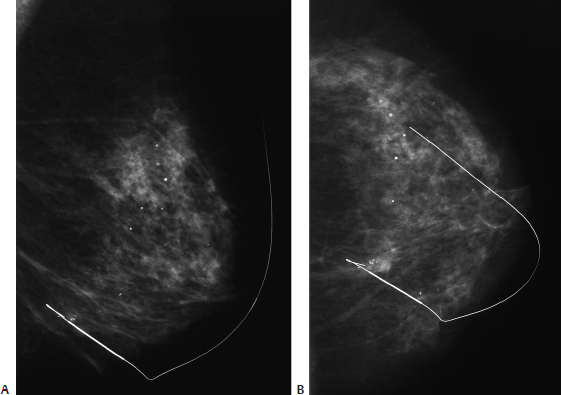
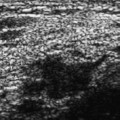
19 Calcifications: Fine Linear/Branching Microcalcifications A 68-year-old woman has increasing calcifications on her screening mammogram. She has a past history of lung cancer and bladder cancer. Stereotactic core needle biopsy of the calcifications was not conclusive, so a needle localization and excisional biopsy were performed. The patient was unable to maintain an upright position for the needle localization, so sonographic guidance of the wire localization was performed. • Normal exam Calcifications (Figs. 19.1 and 19.2) • Type: fine linear/branching • Distribution: linear Fig. 19.1 In the 6 o’clock position of the left breast, there is a nodular density associated with linear calcifications (circle). (A) Left MLO mammogram. (B) Left CC mammogram. (C) Enlargement of circled calcificiations in A. (D) Enlargement of circled calcifications in B. Fig. 19.2 Mammograms performed after sonographic guidance of needle localization demonstrate that the wire is in excellent position with respect to the calcifications. (A) Left ML mammogram after needle localization. (B) Left CC mammogram after needle localization. Frequency • 13 MHz Mass (Fig. 19.3) • Margin: ill defined • Echogenicity: hypoechoic • Retrotumoral acoustic appearance: bilateral edge shadowing • Shape: ellipsoid Fig. 19.3 Left radial breast sonogram. The calcifications identified in Fig. 19.1 corresponded to a focally dilated tubular structure associated with a solid nodule. Both the tubular structure and the nodule contained multiple calcifications (arrows). Sonographic needle localization was performed using this image. After localization, mammo-graphic images were taken to confirm the wire position (Fig. 19.2). • Adenomyoepithelioma • BI-RADS assessment category 4, suspicious abnormality; biopsy should be considered. • Adenomyoepithelioma is an unusual breast tumor that is generally benign but may recur after local excision. Occasionally, carcinoma or malignant myoepithelioma will arise within an adenomyoepithelioma. • Sonographic guidance for needle localization of calcifications is rarely necessary. To perform this procedure, it is critical that one be confident in locating the calcifications. High-frequency sonography is generally a necessity in this situation. Leucht D, Madjar H. Microcalcification in sonography. In: Leucht D, ed. Teaching Atlas of Breast Ultrasound. New York: Thieme, 1996:189–204 Tavassoli FA, Fattaneh A. Pathology of the Breast, 2nd ed. Stamford: Appleton & Lange; 1999:763–791 A 70-year-old woman presents with new right breast calcifications on her screening mammogram. • Normal exam Calcifications (Fig. 19.4) • Type: fine linear/branching • Distribution: grouped/clustered Fig. 19.4 In the inferior outer breast, there is a cluster of heterogeneous calcifications that are arranged in a linear pattern (arrows). (A) Right MLO magnification mammogram. (B) Right exaggerated CC magnification mammogram. • Ductal carcinoma in situ • Solid type with high nuclear grade and high mitotic rate and with comedo necrosis and dystrophic calcifications • BI-RADS assessment category 4, suspicious abnormality; biopsy should be considered. • Calcification in DCIS with comedo necrosis usually occurs in the center of the necrotic tumor debris within the ducts. As a result, the mammographic calcification pattern of this histology is commonly fine linear or branching. However, there is considerable mammographic overlap between the different DCIS subtypes, so histologic subtype cannot be mammographically predicted with great accuracy. Hermann G, Keller RJ, Drossman S, et al. Mammographic pattern of microcalcifications in the preoperative diagnosis of comedo ductal carcinoma in situ: histopathologic correlation. Can Assoc Radiol J 1999;50:235–240 Stomper PC, Connolly JL. Ductal carcinoma in situ of the breast: correlation between mammographic calcification and tumor subtype. AJR Am J Roentgenol 1992;159:483–485 A 45-year-old woman presents for screening mammogram. • Normal exam Calcifications (Fig. 19.5) • Type: linear and branching pleomorphic/heterogeneous • Distribution: segmental Fig. 19.5 In the left upper outer quadrant, there is segmental distribution of linear and branching pleomorphic calcifications. (A) Left ML magnification mammogram. (B) Left CC magnification mammogram.
Case 19.1: Adenoymyoepithelioma
Case History
Physical Examination
Mammogram
Ultrasound
Pathology
Management
Pearls and Pitfalls
Suggested Reading
Case 19.2: Ductal Carcinoma in Situ
Case History
Physical Examination
Mammogram
Pathology
Management
Pearls and Pitfalls
Suggested Reading
Case 19.3: Ductal Carcinoma in Situ
Case History
Physical Examination
Mammogram
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


