Fig. 15.1
Transanal ultrasonographic appearance of an internal rectal fistula (arrows) arising from an ileal cancer and abutting the wall of the distal rectum (N). The presence of neoplastic tissue within the fistuolous tract was not detectable with conventional diagnostic methods and was discovered only after surgery, proctectmy, and fistulectomy
In patients with anorectal cancer presenting with a perianal fistula, imaging diagnosis may be problematic. In this case, transanal ultrasound can be requested to evaluate a palpable mass within the anal canal associated with a perianal fistula. Transanal ultrasound may provide information regarding tumor size, location, depth of the cancer’s mural penetration, and of the tumor extension beyond the anal canal through the perineum and into adjacent structures (Fig. 15.2).
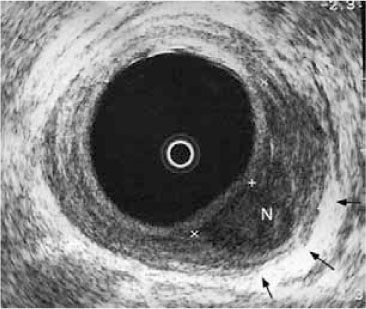
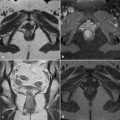
Fig. 15.2
Tumor (N) of the anal canal involving the subepithelium and internal sphincter. The neoplasia is confined to the internal sphincter (arrows), leaving intact the external anal sphincter (stage: T2, N0)
Squamous cell carcinomas of the anal canal are rare but require careful staging to select appropriate treatment, typically with combined chemotherapy and radiotherapy. Transanal ultrasound allows tumor staging based on depth of tumor invasion (Table 15.1), which is useful in determining the response to radiotherapy [12] and in monitoring the patient for local recurrence.
Table 15.1
Ultrasound staging of anal malignancy
Stage | Definition |
|---|---|
T1 | Confined to the subepithelium |
T2 | Limited to the sphincter muscles |
T3 | Penetrating the external anal sphincter |
T4 | Involving adjacent structures |
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


