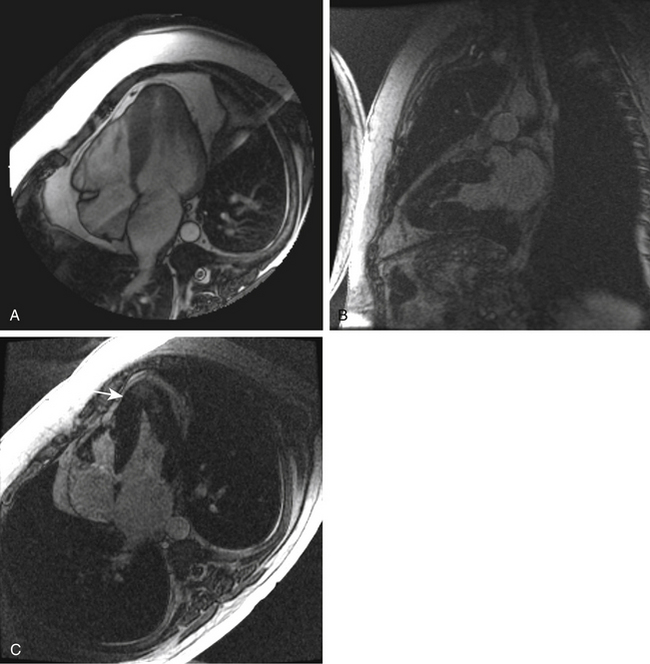
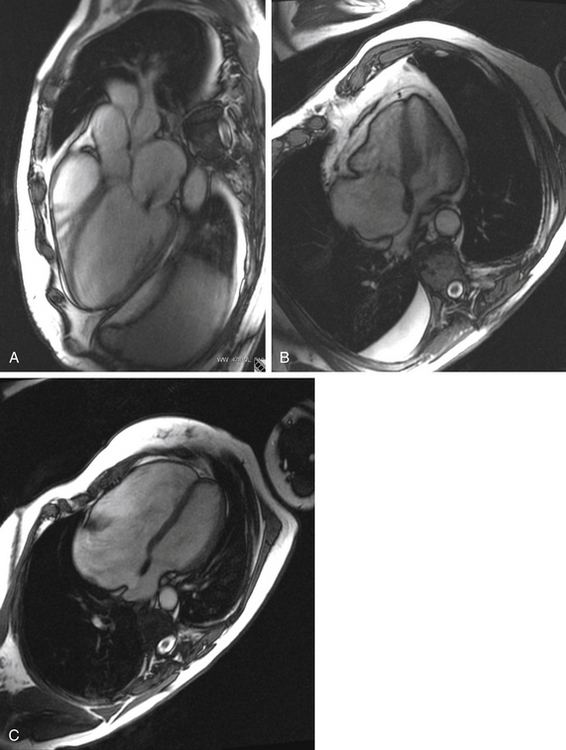
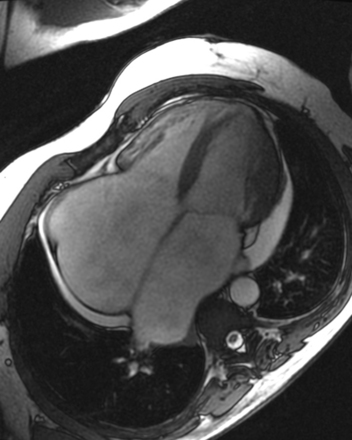
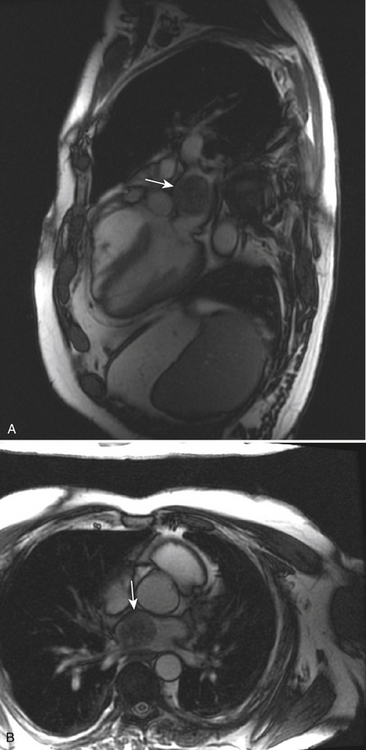
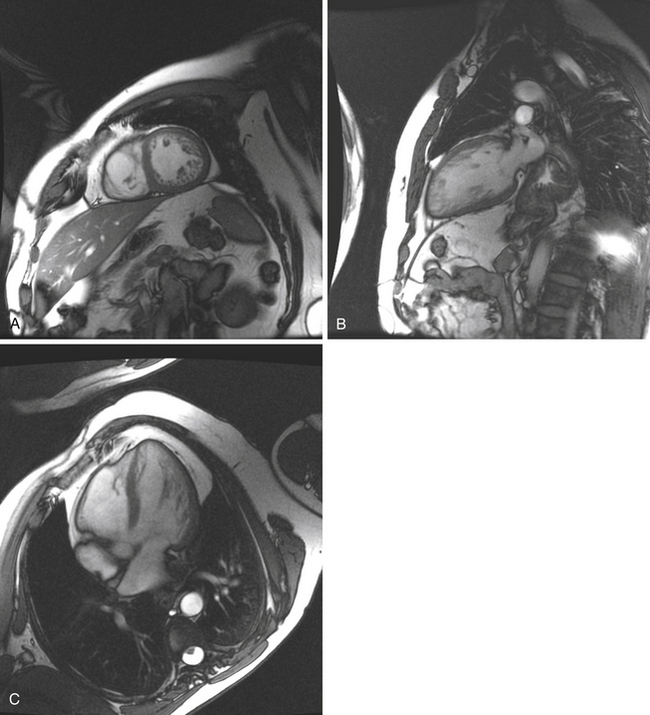
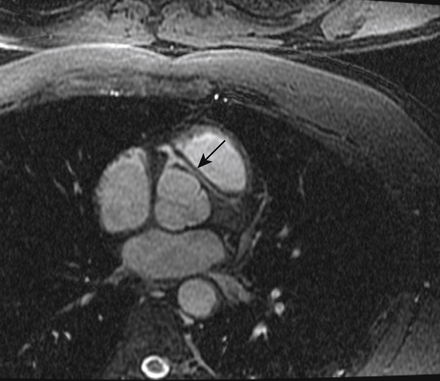
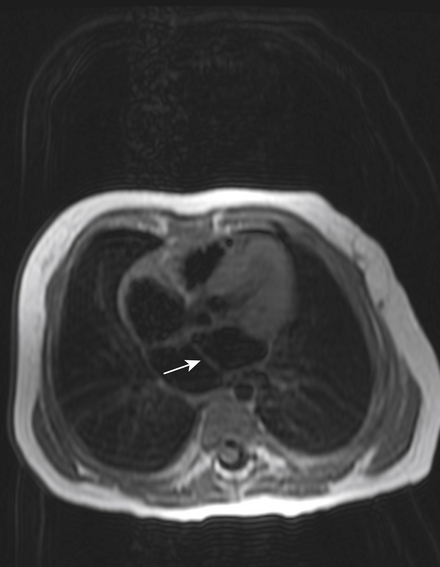
5 Cardiovascular Magnetic Resonance Imaging Adult Cardiac MR Cases FIGURE 5-1 Nonobstructive hypertrophic cardiomyopathy. Cardiac MRI is used to evaluate the severity and location of hypertrophy and fibrosis in HCM. Cine imaging is used to evaluate dynamic outflow tract obstruction from the systolic anterior motion of the anterior mitral valve leaflet. Cardiac MRI was performed to evaluate a 20-year-old white male presenting with worsening exertional dyspnea and near-syncope. His brother died suddenly at age 23. An echocardiogram showed symmetric hypertrophy without evidence of a dynamic outflow tract obstruction. A, The horizontal WB long-axis image shows diffuse hypertrophic changes of the LV walls. Postcontrast vertical (B) and horizontal (C) long-axis images demonstrate areas of hyperenhancement (arrow) from myocardial fibrosis at the cardiac apex. This fibrosis is associated with increased risk of heart failure and sudden death. FIGURE 5-2 Valvular disease. Though echocardiography is the primary imaging modality used to assess valvular structures, regurgitation, and stenosis, cardiac MRI is useful in patients with suboptimal echocardiographic images. Valve leaflet thickness and mobility can be assessed. In addition, quantification of valvular regurgitation may be completed using phase and volumetric techniques. A, Mitral regurgitation. A 72-year-old African American male with longstanding hypertension presented with progressive heart failure. On cardiac MRI, this WB LV inflow view demonstrates an enlarged LV with significant mitral regurgitation, represented by the black jet in the white blood extending from the valve into the left atrium. B, Tricuspid stenosis. A 30-year-old female presented with symptoms of progressive right heart failure, increasing abdominal pain, ascites, and lower extremity edema over the past few months. Cardiac MRI demonstrated a normal RV but thickened tricuspid valve leaflets. The right atrium is markedly enlarged, and an incidental right pleural effusion can be seen on this WB horizontal long-axis view. C, Ebstein anomaly. Cardiac MRI demonstrates a markedly enlarged right atrium and RV on this WB horizontal long-axis view. The tricuspid valve leaflets are not well visualized. The leftward bowing of the atrial septum is consistent with increased right-sided pressures. The patient was a 70-year-old female who presented with a vague history of cardiac murmur and 6-month history of abdominal swelling and lower extremity edema. Echocardiography demonstrated inferior displacement of the septal leaflet of the tricuspid valve, a dilated right atrium and RV, and severe tricuspid regurgitation consistent with Ebstein anomaly. FIGURE 5-3 Restrictive cardiomyopathy. WB horizontal long-axis image obtained from a 60-year-old male whot had felt poorly for several years but had become more dyspneic over the past 3 months. The patient’s history includes Hodgkin lymphoma as a teenager with mantle radiation. Cardiac MRI, completed to help determine if the patient had restrictive cardiomyopathy versus constrictive pericarditis, demonstrated normal LV and RV cavity sizes and systolic function. Both left and right atria are massively enlarged. No significant valvular regurgitation was seen. The pericardium is of normal thickness. The patient was diagnosed with restrictive cardiomyopathy. FIGURE 5-4 Left atrial myxoma. A 45-year-old Native American male evaluated for a several-month history of night sweats and several episodes of positional near-syncope, particularly when he goes bowling. TTE had demonstrated a left atrial mass, and cardiac MRI confirmed that the large left atrial mass occupying the superior portion of the left atrium was a myxoma (arrows). The mass appears homogeneous and smooth with a capsule. WB vertical long-axis (A) and axial (B) images demonstrate the left atrial myxoma. Often, contrast is administered to help differentiate cardiac masses. For example, lymphomas are usually markedly enhancing, whereas myxomas usually do not significantly enhance. FIGURE 5-5 Noncompaction cardiomyopathy. A 35-year-old white female presented with heart failure and no prior cardiac history. TTE was technically challenging, but demonstrated a normal LV size with prominent trabeculations at the apex. WB T2-weighted images in short-axis (A), vertical long-axis (B), and horizontal long-axis (C) demonstrate a thickened LV wall secondary to thickened trabeculations. Blood is clearly viewed within the thick trabeculations. This patient was diagnosed with noncompaction cardiomyopathy. FIGURE 5-6 Anomalous LCA. A 20-year-old African American female presented with recurrent exertional chest pain. This fat-suppressed T2-weighted axial image reveals an abnormal course of the LCA (arrow) between the aorta and main PA trunk. This is a known risk factor for sudden cardiac death in young adults during exercise. The LCA may be compressed between the aorta and PA during episodes of increased cardiac output. FIGURE 5-7 Cor triatriatum sinistrum. A 27-year-old white male presented with dyspnea and a heart murmur. The T1-weighted axial cardiac MRI shown here demonstrates cor triatriatum sinistrum. The left atrium is partitioned into two segments by a fibromuscular membrane (arrow). The posterosuperior portion usually receives the pulmonary venous return, and the anteroinferior portion contains the left atrial appendage and mitral valve. In this image, the LV appears normal in size. The RV is prominent with low normal function on cine imaging. Depending on the presence and size of the communication(s) present, pulmonary hypertension may develop secondary to obstruction of pulmonary venous flow. In symptomatic patients, the membrane can be surgically resected. There are several theories of development of cor triatriatum sinistrum, including malincorporation, malseptation, and entrapment. Adult Congenital MR Cases Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related posts: Cardiovascular Computed Tomography Echocardiography Angiography Electrocardiography INDEX Artificial intelligence in nuclear cardiology Stay updated, free articles. Join our Telegram channel Join Tags: Cardiovascular Imaging Review Expert Consult Dec 26, 2015 | Posted by admin in CARDIOVASCULAR IMAGING | Comments Off on Cardiovascular Magnetic Resonance Imaging Full access? Get Clinical Tree
5 Cardiovascular Magnetic Resonance Imaging Adult Cardiac MR Cases FIGURE 5-1 Nonobstructive hypertrophic cardiomyopathy. Cardiac MRI is used to evaluate the severity and location of hypertrophy and fibrosis in HCM. Cine imaging is used to evaluate dynamic outflow tract obstruction from the systolic anterior motion of the anterior mitral valve leaflet. Cardiac MRI was performed to evaluate a 20-year-old white male presenting with worsening exertional dyspnea and near-syncope. His brother died suddenly at age 23. An echocardiogram showed symmetric hypertrophy without evidence of a dynamic outflow tract obstruction. A, The horizontal WB long-axis image shows diffuse hypertrophic changes of the LV walls. Postcontrast vertical (B) and horizontal (C) long-axis images demonstrate areas of hyperenhancement (arrow) from myocardial fibrosis at the cardiac apex. This fibrosis is associated with increased risk of heart failure and sudden death. FIGURE 5-2 Valvular disease. Though echocardiography is the primary imaging modality used to assess valvular structures, regurgitation, and stenosis, cardiac MRI is useful in patients with suboptimal echocardiographic images. Valve leaflet thickness and mobility can be assessed. In addition, quantification of valvular regurgitation may be completed using phase and volumetric techniques. A, Mitral regurgitation. A 72-year-old African American male with longstanding hypertension presented with progressive heart failure. On cardiac MRI, this WB LV inflow view demonstrates an enlarged LV with significant mitral regurgitation, represented by the black jet in the white blood extending from the valve into the left atrium. B, Tricuspid stenosis. A 30-year-old female presented with symptoms of progressive right heart failure, increasing abdominal pain, ascites, and lower extremity edema over the past few months. Cardiac MRI demonstrated a normal RV but thickened tricuspid valve leaflets. The right atrium is markedly enlarged, and an incidental right pleural effusion can be seen on this WB horizontal long-axis view. C, Ebstein anomaly. Cardiac MRI demonstrates a markedly enlarged right atrium and RV on this WB horizontal long-axis view. The tricuspid valve leaflets are not well visualized. The leftward bowing of the atrial septum is consistent with increased right-sided pressures. The patient was a 70-year-old female who presented with a vague history of cardiac murmur and 6-month history of abdominal swelling and lower extremity edema. Echocardiography demonstrated inferior displacement of the septal leaflet of the tricuspid valve, a dilated right atrium and RV, and severe tricuspid regurgitation consistent with Ebstein anomaly. FIGURE 5-3 Restrictive cardiomyopathy. WB horizontal long-axis image obtained from a 60-year-old male whot had felt poorly for several years but had become more dyspneic over the past 3 months. The patient’s history includes Hodgkin lymphoma as a teenager with mantle radiation. Cardiac MRI, completed to help determine if the patient had restrictive cardiomyopathy versus constrictive pericarditis, demonstrated normal LV and RV cavity sizes and systolic function. Both left and right atria are massively enlarged. No significant valvular regurgitation was seen. The pericardium is of normal thickness. The patient was diagnosed with restrictive cardiomyopathy. FIGURE 5-4 Left atrial myxoma. A 45-year-old Native American male evaluated for a several-month history of night sweats and several episodes of positional near-syncope, particularly when he goes bowling. TTE had demonstrated a left atrial mass, and cardiac MRI confirmed that the large left atrial mass occupying the superior portion of the left atrium was a myxoma (arrows). The mass appears homogeneous and smooth with a capsule. WB vertical long-axis (A) and axial (B) images demonstrate the left atrial myxoma. Often, contrast is administered to help differentiate cardiac masses. For example, lymphomas are usually markedly enhancing, whereas myxomas usually do not significantly enhance. FIGURE 5-5 Noncompaction cardiomyopathy. A 35-year-old white female presented with heart failure and no prior cardiac history. TTE was technically challenging, but demonstrated a normal LV size with prominent trabeculations at the apex. WB T2-weighted images in short-axis (A), vertical long-axis (B), and horizontal long-axis (C) demonstrate a thickened LV wall secondary to thickened trabeculations. Blood is clearly viewed within the thick trabeculations. This patient was diagnosed with noncompaction cardiomyopathy. FIGURE 5-6 Anomalous LCA. A 20-year-old African American female presented with recurrent exertional chest pain. This fat-suppressed T2-weighted axial image reveals an abnormal course of the LCA (arrow) between the aorta and main PA trunk. This is a known risk factor for sudden cardiac death in young adults during exercise. The LCA may be compressed between the aorta and PA during episodes of increased cardiac output. FIGURE 5-7 Cor triatriatum sinistrum. A 27-year-old white male presented with dyspnea and a heart murmur. The T1-weighted axial cardiac MRI shown here demonstrates cor triatriatum sinistrum. The left atrium is partitioned into two segments by a fibromuscular membrane (arrow). The posterosuperior portion usually receives the pulmonary venous return, and the anteroinferior portion contains the left atrial appendage and mitral valve. In this image, the LV appears normal in size. The RV is prominent with low normal function on cine imaging. Depending on the presence and size of the communication(s) present, pulmonary hypertension may develop secondary to obstruction of pulmonary venous flow. In symptomatic patients, the membrane can be surgically resected. There are several theories of development of cor triatriatum sinistrum, including malincorporation, malseptation, and entrapment. Adult Congenital MR Cases Only gold members can continue reading. Log In or Register to continue Share this: Share on X (Opens in new window) X Share on Facebook (Opens in new window) Facebook Related posts: Cardiovascular Computed Tomography Echocardiography Angiography Electrocardiography INDEX Artificial intelligence in nuclear cardiology Stay updated, free articles. Join our Telegram channel Join Tags: Cardiovascular Imaging Review Expert Consult Dec 26, 2015 | Posted by admin in CARDIOVASCULAR IMAGING | Comments Off on Cardiovascular Magnetic Resonance Imaging Full access? Get Clinical Tree