Chapter 2 Second Trimester Obstetrics
Karen Tran-Harding
2 Questions and Answers
Refer to the following figure for questions 2.1 to 2.3.

Question 2.1: What measurement is being obtained?
Nuchal fold.
Nuchal translucency.
Skull thickness.
Biparietal diameter.
Question 2.2: At what gestational age is the measurement usually obtained?
At 8 to 11 weeks.
At 11 to 14 weeks.
At 15 to 20 weeks.
At 22 to 25 weeks.
Question 2.3: Which of the following is seen on this image?
Lemon skull and banana sign.
Strawberry skull and banana sign.
Lemon skull and Spalding sign.
Strawberry skull and Spalding sign.
Answer 2.1:
A. Correct. The image demonstrates measurement of the nuchal fold. This is typically obtained in the midline, at the level of the posterior fossa. The nuchal fold is considered abnormal if it is 6 mm or greater. Increased nuchal skin thickness is a sensitive ultrasound marker for trisomy 21.
B. Incorrect. The nuchal translucency measurement is obtained more inferiorly at the level of the neck.
C, D—Incorrect. The nuchal fold is being measured.
Answer 2.2:
C. Correct. While there is some variation in the literature, the nuchal fold is obtained in the second trimester between 15 to 18–20 weeks.
A, B, D—Incorrect.
Answer 2.3:
A. Correct. The image demonstrates scalloping of the frontal bones resulting in a lemon-like shape of the skull. There is also bowing of the cerebellum with effacement of the cisterna magna. The cerebellar shape becomes reminiscent of a banana. These findings are typically encountered in Chiari II malformation and spina bifida.
B. Incorrect. Strawberry skull is seen as flattening of the occiput due to midbrain hypoplasia and flattening of the frontal bones due to frontal lobe hypoplasia. This is associated with trisomy 18.
C. Incorrect. Spalding sign is characterized by overlapping skull bones and is encountered in situations of fetal demise.
D. Incorrect. Strawberry skull and Spalding sign are not depicted in the image presented.
Question 2.4: Which of the following is true about the anomaly seen on ultrasound (US)?

It is formed by infolding of the neuroepithelium and is lined by epithelium.
It is associated with trisomy 13.
Other anomalies should be sought including overlapping digits and rocker bottom deformity.
When this anomaly is seen, the next step is an amniocentesis for definitive diagnosis.
Answer:
C. Correct. The image demonstrates the classic appearance of a choroid plexus cyst, a frequent finding, though often of little clinical significance. However, there is an association with trisomy 18. For this reason, overlapping digits and rocker bottom feet should be excluded on prenatal sonographic evaluation.
A. Incorrect. Although choroid plexus cysts are formed by infolding of the neuroepithelium, it is not a true cyst and is not lined by epithelium. Rather, choroid plexus cysts are formed from spaces within the choroid plexus and are filled with clear fluid (CSF) and cellular debris.
B. Incorrect. Associations with choroid plexus cysts include trisomy 18, trisomy 21, Klinefelter’s syndrome, and Aicardi syndrome. Trisomy 13 is not a known association.
D. Incorrect. Although choroid plexus cysts can be associated with chromosomal abnormalities, these can be isolated findings as well. When a choroid plexus is seen, the next best step is a triple screen.
Question 2.5: Which of the following is true given the abnormality seen on the US image? The arrow points to the fetal bladder.

Other major anomalies or aneuploidies are rare.
This anomaly is typically located to the right of umbilical cord insertion.
The stomach bubble should still be visible within the abdomen.
The abdominal contents are only covered by a two-layer sac of amnion and peritoneum.
Answer:
D. Correct. The image demonstrate the classic appearance of an omphalocele, seen to the right of the image as herniated abdominal contents covered by a membrane. This membrane consists of two layers, amnion and peritoneum.
A. Incorrect. This anomaly is associated with other major anomalies or aneuploidies in over 50% of cases.
B. Incorrect. The umbilical cord inserts into the anterior part of the defect in omphaloceles.
C. Incorrect. Like gastroschisis and congenital diaphragmatic hernias, omphaloceles are associated with absence of the stomach bubble within the abdomen.
Question 2.6: What is true about the condition demonstrated within this sonographic image?

Associated anomalies and aneuploidies are rare.
It is the most common anterior abdominal wall defect of the fetus.
The umbilical cord inserts into the anterior part of the defect.
Fetal ascites is a common association.
Answer:
A. Correct. The image demonstrates the classic appearance of gastroschisis, with herniated abdominal contents seen to the left of the image. Associated anomalies and aneuploidies are rare.
B. Incorrect. Omphaloceles are the most common anterior abdominal wall defect of the fetus occurring in 1 in 4,000 live births. Gastroschisis occurs in 1 in 10,000 live births.
C. Incorrect. The umbilical cord inserts normally on the abdomen. The defect is usually to the right of the umbilicus. The umbilical cord inserts into the anterior part of the defect in omphaloceles.
D. Incorrect. Fetal ascites cannot occur in gastroschisis as the bowel is not covered by a membrane and floats freely in the amniotic fluid.
Question 2.7: What is true of this condition?

It is almost always unilateral.
It is a feared complication of early amniocentesis.
It does not occur in dizygotic twin gestations.
It is often seen in the setting of polyhydramnios.
Answer:
B. Correct. The image demonstrates the classic appearance of talipes equinovarus (clubfoot). Visualizing the tibia/fibula and metatarsals/phalanges on the same image is helpful in making the diagnosis on prenatal ultrasound. It is a feared complication of early amniocentesis and associated with a four-fold increase of talipes equinovarus (clubfoot) compared with chorionic villous sampling.
A. Incorrect. Clubfoot may frequently affect one or both feet.
C. Incorrect. Clubfoot may occur in any type of multifetal gestation secondary to fetal crowding.
D. Incorrect. Clubfoot is often seen in the setting of oligohydramnios, presumably caused by fixed positioning of fetal extremities due to lack of movement.
Question 2.8: Which of the following is correct regarding the imaged condition?

It is characterized by excess fluid in at least two body compartments.
Pericardial effusions are uncommon in this condition.
In the immune-mediated variety, it is most often caused by ABO blood type incompatibility.
Oligohydramnios is a frequent association.
Answer:
A. Correct. The images demonstrate pleural effusions and skin thickening/edema consistent with fetal hydrops. Fetal hydrops is characterized by excess fluid in at least two body compartments.
B. Incorrect. Pleural and pericardial effusions as well as ascites are typical findings.
C. Incorrect. The most common cause for the immune mediated type of fetal hydrops is rhesus (Rh) incompatibility.
D. Incorrect. Fetal hydrops is more likely to be associated with polyhydramnios.
Question 2.9: The kidneys are indicated by the arrows. What is true of the finding depicted in the kidney to the left of the image?

The renal changes occur secondary to obstruction or atresia at the level of the distal ureter.
The condition is characterized by multiple communicating cysts.
Renal cysts can be a normal finding in utero.
The amniotic fluid level is usually normal.
Answer:
D. Correct. The image demonstrates multiple cysts within the kidney to the left of the image. The renal parenchyma is also somewhat echogenic. The findings are consistent with multicystic dysplastic kidney (MCDK). Amniotic fluid level is usually normal in MCDK.
A. Incorrect. The renal changes of MCDK occur secondary to obstruction at the renal pelvis or the proximal ureter prior to 10 weeks.
B. Incorrect. MCDK is characterized by noncommunicating cysts that also do not communicate with the renal pelvis. Rather, ureteropelvic junction (UPJ) obstruction demonstrates fluid areas that connect, i.e., pelvocaliectasis.
C. Incorrect. MCDK occurs more often unilaterally. Bilateral MCDK can be lethal owing to oligohydramnios and pulmonary hypoplasia.
Question 2.10: Which of the following is correct about the condition depicted in the image?

This condition is uniformly fatal in utero or within the first year of life.
This disease typically presents during the first trimester.
Pulmonary hypoplasia is a known complication.
The amniotic fluid level is usually normal.
Answer:
C. Correct. This sonographic image depicts bilaterally enlarged echogenic kidneys, filling much of the abdominal cavity. These findings are typical of autosomal recessive polycystic kidney disease (ARP-KD). There is often associated oligohydramnios with thoracic hypoplasia. The narrowed thorax is noted within the right side of the sonographic image.
A. Incorrect. The juvenile form of ARPKD may result in a longer life expectancy. However, associated liver fibrosis leads to severe portal hypertension in adolescence/early adulthood.
B. Incorrect. The typical prenatal sonographic findings are usually detected during the second and third trimesters.
D. Incorrect. Oligohydramnios is associated with ARPKD.
Question 2.11: What is true about the measurement being obtained?

This measurement should be obtained between 15- and 18-week gestational age.
The measurement should be obtained with mild neck flexion.
A measurement of greater than 3 mm is abnormal.
An unfused amnion may lead to underestimation.
Answer:
C. Correct. The image demonstrates measurement of the nuchal translucency. This measurement is obtained at 11- to 14-week gestational age. The measurement is obtained from inner echogenic line to inner echogenic line, at the level of the neck, with the neck in neutral position. A measurement of greater than 3 mm is abnormal and signifies an increased risk for chromosomal abnormalities such as trisomy 21.
A. Incorrect. The nuchal translucency is measured between 11- and 14-week gestational age, earlier than the nuchal fold which is measured between 15 and 18–20 weeks.
B. Incorrect. The measurement of the nuchal translucency is at the level of the neck. The nuchal fold is measured at the level of the cerebellum and cisterna magna.
D. Incorrect. An unfused amnion may lead to overestimation of the nuchal translucency as the unfused amnion may be mistaken for the fetal skin line.
Question 2.12: What is true about the finding depicted in the following image?

It represents calcification of the chordae tendineae.
This finding should always prompt a karyotype analysis.
The most common location for this finding is the right ventricle.
The salient finding does not usually cause shadowing.
Answer:
D. Correct. The sonographic image depicts an echogenic cardiac spot. These spots represent mineralization of the papillary muscle and they typically do not cast a shadow. This is likely related to their small size (usually 3 mm or less) and constant motion.
A. Incorrect. It represents mineralization of the papillary muscle.
B. Incorrect. Although the echogenic cardiac spot may be a soft marker for trisomy 21, in a low-risk population, the mildly increased risk of Down’s syndrome does not require a karyotype analysis.
C. Incorrect. The most common location for this finding is the left ventricle.
Question 2.13: What is true about the finding depicted in the following image?

This anomaly affects females more often than males.
The finding is often bilateral when associated with holoprosencephaly.
Oligohydramnios is a common associated finding.
Fifty percent of patients with this condition will have other structural anomalies.
Answer:
D. Correct. The image demonstrates the classic appearance of cleft palate/lip. Approximately 50% of patients with this condition have other anomalies, such as trisomy 13 and 18. Both cleft lip and palate is found in 50%, isolated cleft lip in 20%, and isolated cleft palate in 30%.
A. Incorrect. This anomaly affects males more than females, accounting for 60 to 80% of cases.
B. Incorrect. Midline defects are often associated with holoprosencephaly.
C. Incorrect. These pregnancies are often complicated by polyhydramnios due to impaired fetal swallowing.
Question 2.14: What is true of the finding depicted in the following images?

Turner’s syndrome is the most common association.
About 20% of patients will have an associated chromosomal abnormality.
This abnormality is caused by venous dysplasia.
These are only seen in the posterior neck of the fetus.
Answer:
A. Correct. The images demonstrate a large septated cystic structure arising from the posterior neck. These findings are typical of cystic hygroma. Turner’s syndrome is the most common association.
B. Incorrect. About 70% of patients will have an associated chromosomal abnormality.
C. Incorrect. This abnormality is caused by lymphatic dysplasia with subsequent leakage of the lymphatics causing localized areas of fluid collections.
D. Incorrect. Cystic hygromas can be seen elsewhere in the body including the thoracic and abdominal walls.
Question 2.15: Which is true of the finding depicted in the image below?

It is usually the earliest finding of cystic fibrosis.
The cause for this finding typically originates within the colon.
Oligohydramnios is usually present.
The disease that most often causes this finding is autosomal dominant.
Answer:
A. Correct. The image demonstrates a dilated segment of bowel. Almost all infants with dilated bowel and meconium ileus have cystic fibrosis. Dilated bowel is typically the earliest finding of cystic fibrosis.
B. Incorrect. Dilated proximal small bowel caused by thick and sticky meconium usually occurs in the terminal ileum rather than the colon.
C. Incorrect. The amniotic fluid level is usually normal or high.
D. Incorrect. Cystic fibrosis is an autosomal recessive inherited disease.
Question 2.16: Which of the following is true of the imaged condition below?

The diagnosis should be delayed until the early second trimester.
Oligohydramnios is a frequent finding.
The face below the orbits is usually malformed.
High maternal serum beta human chorionic gonadotropin level is usually present in the second trimester.
Answer:
A. Correct. The image demonstrates lack of supra-orbital tissue consistent with anencephaly. By 12 to 14 weeks, the normal fetal head and intracranial structures can be identified. Although some of these structures can be identified via a transvaginal scan as early as 9 to 10 weeks, the definitive diagnosis of anencephaly should be made in the early second trimester.
B. Incorrect. Polyhydramnios is usually found in cases of anencephaly secondary to impaired fetal swallowing.
C. Incorrect. Although there is absence of the normal calvarium and normal brain tissue above the orbits, the face below the orbits is usually normal.
D. Incorrect. High maternal serum alpha fetoprotein level is present in the second trimester.
Question 2.17: Regarding the finding below, which statement is correct?

This finding is within normal limits.
The upper limit for lateral ventricular diameter is 10 mm in the second trimester and 20 mm in the third trimester.
The fetal prognosis is related to the cerebral cortical thickness.
A small amount of fluid between the choroid plexus and medial wall of the lateral ventricle is diagnostic for hydrocephalus between 18- and 20-week gestation.
Answer:
C. Correct. The image demonstrates severe ventriculomegaly with the classic dangling choroid plexus sign. Fetal prognosis is related to the cerebral cortical thickness.
A. Incorrect. The imaged findings are grossly abnormal.
B. Incorrect. The upper limit for lateral ventricular diameter is 10 mm throughout pregnancy.
D. Incorrect. Between 18- and 20-week gestation, a small amount of fluid between the medial wall of the lateral ventricle and the choroid plexus can be a normal finding.
Question 2.18: This sonographic image was obtained at the level of the upper abdomen. What chromosomal abnormality is most likely to be present?

Trisomy 13.
Trisomy 18.
Trisomy 21.
Meckel–Gruber syndrome.
Answer:
C. Correct. The image demonstrates the classic “double bubble sign” the hallmark of duodenal atresia. Trisomy 21 is the most common chromosomal abnormality that is associated duodenal atresia.
A. Incorrect. Trisomy 13 is not typically associated with duodenal atresia.
B. Incorrect. Trisomy 18 is also not typically associated with duodenal atresia.
D. Incorrect. MeckelGruber syndrome is not typically associated with duodenal atresia.
Question 2.19: This sonographic image was obtained at the lower uterine segment in the second trimester of a 32-year-old female. What finding is demonstrated?

Cervical incompetence.
Placenta previa.
Cervical polyp.
Premature rupture of membranes.
Answer:
A. Correct. The image demonstrates a longitudinal view of the cervix showing funneling and shortening of the cervix consistent with cervical incompetence.
B. Incorrect. The placenta is not imaged.
C. Incorrect. A cervical polyp is not present.
D. Incorrect. Cervical incompetence is associated with premature rupture of membranes (PROM). The main sonographic manifestation of PROM is oligohydramnios or anhydramnios.
Question 2.20: What is the normal cervical length in pregnancy?
At least 2 cm.
At least 3 cm.
At least 4 cm.
At least 5 cm.
Answer:
B. Correct. The cervix should be at least 3 cm in length in pregnancy.
A, C, D—Incorrect.
Question 2.21: What finding is depicted in this sonogram of the lower uterine?

Marginal placenta previa.
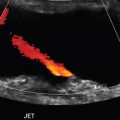
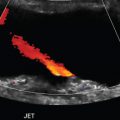
Vasa previa.
Partial placenta previa.
Placental abruption.
Answer:
A. Correct. This image demonstrates the lower edge of the placenta approximating but not covering the internal os. This is consistent with marginal placenta previa.
B. Incorrect. Vasa previa is characterized by placental vessels traversing the internal os and is usually associated with a succenturiate lobe of the placenta and velamentous cord insertion. This condition may be complicated by hemorrhage from the fetal circulation and retained placenta.
C. Incorrect. In partial placenta previa the placenta covers the cervical os, albeit, incompletely.
D. Incorrect. Placental abruption is characterized by premature separation of the placenta from the uterus. This is not demonstrated in the provided image.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


