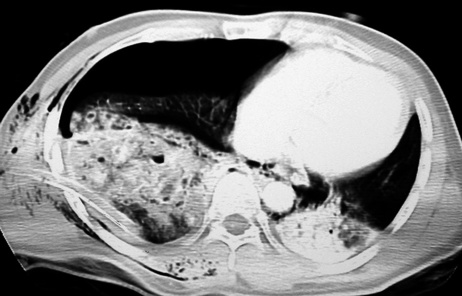
• More than 50% of acute fractures are missed on the initial CXR • Fractures of the 1st to 3rd ribs imply a severe traumatic force and may be associated with vascular, brachial plexus, spinal, or tracheobronchial injuries • Fractures of the 10th to 12th ribs (often better seen on an AXR) are associated with injuries to the liver, spleen or kidneys • Rib fractures are uncommon in children due to their greater inherent elasticity (if present they are usually of the greenstick variety) • Flail segment: double fractures of ≥3 adjacent ribs (or adjacent combined rib, sternal and costochondral fractures) resulting in a segment of chest wall moving paradoxically during the respiratory cycle • This is commonly seen in major trauma victims (20–30%) • Shock waves can lead to microvessel rupture with intra-alveolar and interstitial haemorrhage, as well as alveolar and interstitial oedema • Opacities appear within 6 h of impact and typically clear within 3–10 days (shadowing increasing over the days following admission is unlikely to be due to a simple contusion but may be due to infection, aspiration, fat embolism or ARDS) • Subpleural sparing: there may be an outer 1–2 mm rim of uniformly non-opacified subpleural lung (this is because blood is forced out of the subpleural tissues at the moment of impact)
Chest trauma
CHEST WALL AND LUNG TRAUMA
CHEST WALL AND LUNG TRAUMA
Rib fractures
 additional lateral or oblique views are inappropriate in an acute trauma patient – the main priority is to detect complications such as a pneumothorax, haemothorax, or a pulmonary contusion
additional lateral or oblique views are inappropriate in an acute trauma patient – the main priority is to detect complications such as a pneumothorax, haemothorax, or a pulmonary contusion
 further imaging of these organs is mandatory
further imaging of these organs is mandatory
 there can therefore be significant intrathoracic injury without an associated rib fracture
there can therefore be significant intrathoracic injury without an associated rib fracture
 Multiple fractures (particularly of the posterior ribs) should raise the possibility of non-accidental injury
Multiple fractures (particularly of the posterior ribs) should raise the possibility of non-accidental injury
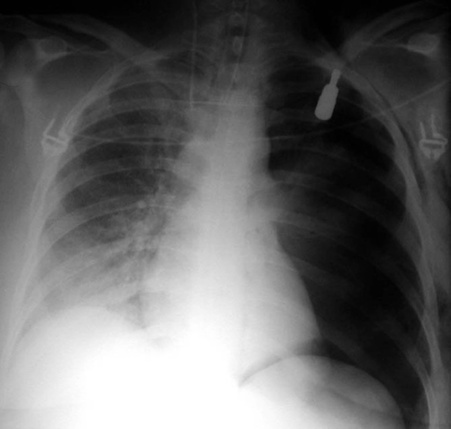
Pneumothorax
 it can result from a pulmonary laceration from a fractured rib fragment or due to a sudden rise in intra-alveolar pressure
it can result from a pulmonary laceration from a fractured rib fragment or due to a sudden rise in intra-alveolar pressure  detection is important as a small pneumothorax can rapidly increase in size with positive-pressure ventilation
detection is important as a small pneumothorax can rapidly increase in size with positive-pressure ventilation
Pulmonary contusion
 ‘contre-coup’ injuries can be seen
‘contre-coup’ injuries can be seen
CXR/CT

 diagnosis is made on a lateral CXR or CT
diagnosis is made on a lateral CXR or CT around ⅓ will have associated spinal cord injuries with a neurological deficit
around ⅓ will have associated spinal cord injuries with a neurological deficit these are usually small (2–5cm) and typically resolve over a few months
these are usually small (2–5cm) and typically resolve over a few months the lung herniates through a defect caused by either rib fractures or shoulder girdle dislocation
the lung herniates through a defect caused by either rib fractures or shoulder girdle dislocation  most are treated conservatively
most are treated conservatively there is delayed development of poorly defined opacities at 48
there is delayed development of poorly defined opacities at 48