These are most commonly an osteomyelitis or a neoplastic disease • Malignant rib tumours: these are commonly metastatic deposits or myeloma • Osteomyelitis: this is uncommon • Pleural thickening usually represents an organized end stage of infective or non-infective inflammation • If generalized and gross it is termed a fibrothorax and may cause significant ventilatory impairment • A localized fibrous tumour of the pleura (⅔ are benign)
Chest wall and pleura
CHEST WALL: BONY AND SOFT TISSUE LESIONS
RIB LESIONS
Aggressive
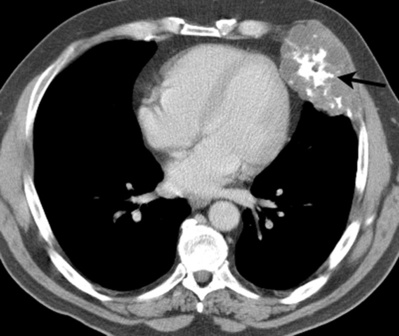
Destructive rib lesions
 primary malignant tumours are rare (but usually a chondrosarcoma)
primary malignant tumours are rare (but usually a chondrosarcoma)
 it may be due to haematogenous spread (e.g. staphylococcal or tuberculous), or it may be caused by direct spread from the lung or pleural space (e.g. actinomycosis)
it may be due to haematogenous spread (e.g. staphylococcal or tuberculous), or it may be caused by direct spread from the lung or pleural space (e.g. actinomycosis)
DIFFERENTIAL OF RIB NOTCHING
Inferior rib notching
Arterial: Coarctation of the aorta, aortic thrombosis, subclavian obstruction, any cause of pulmonary oligaemia
Venous: Superior vena cava obstruction
Arteriovenous: Pulmonary arteriovenous malformation, chest wall arterial malformation
Neurogenic: Neurofibromatosis (ribbon ribs)
Superior rib notching
Connective tissue diseases: Rheumatoid arthritis, SLE, Sjögren’s, scleroderma
Metabolic: Hyperparathyroidism
Miscellaneous: Neurofibromatosis, restrictive lung disease, poliomyelitis, Marfan’s syndrome, osteogenesis imperfecta, progeria
DISEASES OF THE PLEURA
PLEURAL THICKENING AND FIBROTHORAX
DEFINITION
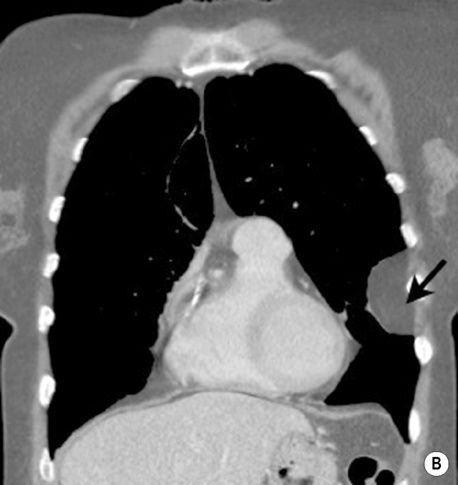
LOCALIZED FIBROUS TUMOUR (LOCALIZED MESOTHELIOMA)
DEFINITION
 there is no relation to previous asbestos exposure
there is no relation to previous asbestos exposure
 they are occasionally associated with syndromes (e.g. basal cell naevus syndrome) or other anomalies (e.g. Sprengel’s deformity)
they are occasionally associated with syndromes (e.g. basal cell naevus syndrome) or other anomalies (e.g. Sprengel’s deformity) it can cause a thoracic outlet syndrome and is often bilateral and asymmetrical
it can cause a thoracic outlet syndrome and is often bilateral and asymmetrical they are most commonly cartilaginous tumours (e.g. a chondroma or osteochondroma)
they are most commonly cartilaginous tumours (e.g. a chondroma or osteochondroma)  they are predominantly found in an anterior location and may show characteristic cartilaginous calcification
they are predominantly found in an anterior location and may show characteristic cartilaginous calcification histiocytosis X
histiocytosis X  haemangioma
haemangioma  aneurysmal bone cyst
aneurysmal bone cyst MRI can determine the extent of a Pancoast’s tumour (and assess the relationship between the tumour and the plexus brachialis)
MRI can determine the extent of a Pancoast’s tumour (and assess the relationship between the tumour and the plexus brachialis)



 it is accompanied by ipsilateral hand and arm anomalies (particularly syndactyly)
it is accompanied by ipsilateral hand and arm anomalies (particularly syndactyly) soft tissue components suggest a liposarcoma
soft tissue components suggest a liposarcoma T2WI: intermediate SI (and low SI with fat suppression)
T2WI: intermediate SI (and low SI with fat suppression) widened intervertebral foramina
widened intervertebral foramina T2WI: high SI
T2WI: high SI  T1WI + Gad: marked contrast enhancement
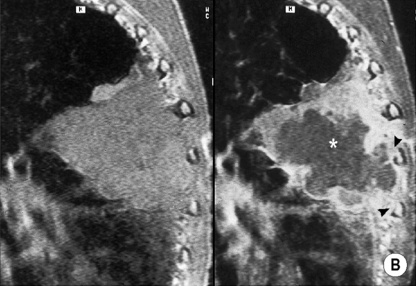
T1WI + Gad: marked contrast enhancement there may be bone remodelling and hypertrophy
there may be bone remodelling and hypertrophy there are signal inhomogeneities generated by vessels, soft tissue and haemorrhage
there are signal inhomogeneities generated by vessels, soft tissue and haemorrhage T2WI: high SI
T2WI: high SI the most common are lipo- or fibrosarcomas
the most common are lipo- or fibrosarcomas it may be an isolated abnormality or associated with other disorders such as Marfan’s syndrome or congenital heart disease (particularly an ASD)
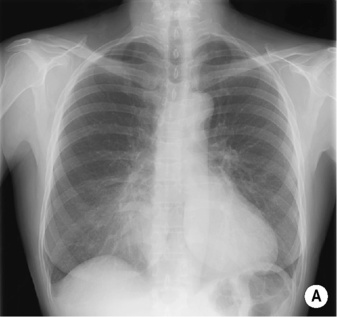
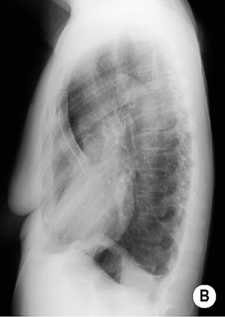
it may be an isolated abnormality or associated with other disorders such as Marfan’s syndrome or congenital heart disease (particularly an ASD) PA CXR: leftward shift of the heart
PA CXR: leftward shift of the heart  an indistinct right heart border simulating middle lobe disease (the sternum replaces aerated lung at the right heart border)
an indistinct right heart border simulating middle lobe disease (the sternum replaces aerated lung at the right heart border)  a steep inferior slope of the anterior ribs
a steep inferior slope of the anterior ribs  undue clarity of the lower dorsal spine seen through the heart
undue clarity of the lower dorsal spine seen through the heart chondrosarcoma
chondrosarcoma  lymphoma
lymphoma  metastatic carcinoma
metastatic carcinoma histiocytosis X
histiocytosis X  Paget’s disease
Paget’s disease  fibrous dysplasia
fibrous dysplasia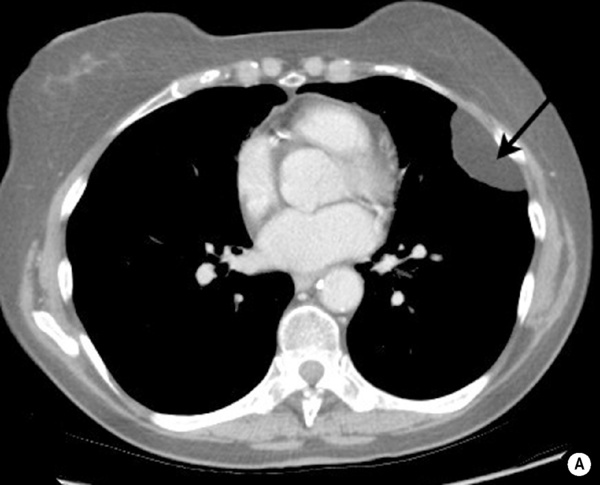



 tuberculosis
tuberculosis  haemorrhagic effusions
haemorrhagic effusions costophrenic angle blunting is common
costophrenic angle blunting is common US is only reliable if this is > 1cm thick
US is only reliable if this is > 1cm thick pleural thickening is seen particularly on the medial rib aspect
pleural thickening is seen particularly on the medial rib aspect an asbestos-related fibrothorax is usually bilateral and rarely calcified
an asbestos-related fibrothorax is usually bilateral and rarely calcified it should be distinguished from a Pancoast’s tumour (if in doubt perform a CT or MRI)
it should be distinguished from a Pancoast’s tumour (if in doubt perform a CT or MRI) it can be diffuse but is more often multifocal and often calcified
it can be diffuse but is more often multifocal and often calcified  it is most commonly found along the lower thorax and diaphragmatic pleura
it is most commonly found along the lower thorax and diaphragmatic pleura they may be calcified
they may be calcified







