• Lobar collapse: this is divided into those causes due to an endobronchial obstruction (intrinsic or extrinsic) or those causes without obstruction • Common causes differ between adults and children: • Subsegmental atelectasis (linear or plate atelectasis): this describes atelectasis involving less than a whole segment • Increased opacity of the affected lobe: this is due to retained secretions and a reduction in lobe aeration • Silhouette sign: this describes loss of an air–soft tissue interface when a segment of collapsed lung abuts an adjacent soft tissue structure (e.g. a heart border) • Direct signs of volume loss: fissure displacement • Indirect signs of volume loss: compensatory shifts of adjacent structures (e.g. hyperinflation of the remaining lobes in proportion to the degree of volume loss) • Ancillary features: absence of air bronchograms within an affected lobe should raise the possibility of a central obstructing lesion • Accurate delineation of a tumour mass from surrounding collapsed lung can be difficult but collapsed lung will usually enhance more than a tumour (the maximal difference is seen between 40 s and 2 min post IV injection) • CT mucous bronchogram sign: tubular, low attenuation branching airways that are dilated with inspissated secretions and seen within the enhancing collapsed lobe (post IV contrast administration) – this is highly suggestive of an obstructing lesion causing lobar collapse • Potential pitfalls: air bronchograms may be seen in peripheral collapsed lobes (due to collateral air drift or tumour necrosis)
Pulmonary lobar collapse
MECHANISMS AND RADIOGRAPHIC APPEARANCES
MECHANISMS AND CAUSES OF LOBAR COLLAPSE
 A segment of atelectatic lung pivots around the central hilum via its attaching bronchovascular structures – any fissures will also influence the direction of collapse
A segment of atelectatic lung pivots around the central hilum via its attaching bronchovascular structures – any fissures will also influence the direction of collapse
 Adults: intrinsic obstruction is commonly due to a bronchogenic tumour (especially in middle-aged or elderly smokers) or mucous plugs
Adults: intrinsic obstruction is commonly due to a bronchogenic tumour (especially in middle-aged or elderly smokers) or mucous plugs
 it is usually a thin horizontal linear opacity abutting the pleura
it is usually a thin horizontal linear opacity abutting the pleura
RADIOGRAPHIC CONSIDERATIONS
 displacement and crowding of the pulmonary vessels and bronchi
displacement and crowding of the pulmonary vessels and bronchi
 Upper lobe collapse: hilar elevation
Upper lobe collapse: hilar elevation  the ipsilateral main bronchus becomes more horizontally orientated
the ipsilateral main bronchus becomes more horizontally orientated
 the contralateral lung may extend across the midline
the contralateral lung may extend across the midline  the anterior junctional line is displaced to the contralateral side
the anterior junctional line is displaced to the contralateral side  displacement of the azygo-oesophageal or posterior junctional lines on a PA CXR
displacement of the azygo-oesophageal or posterior junctional lines on a PA CXR  rib crowding
rib crowding
 A juxtaphrenic diaphragmatic peak: this describes a small triangular density at the highest point of the hemidiaphragm dome with upper lobe (± middle lobe) collapse – this is a useful ancillary sign
A juxtaphrenic diaphragmatic peak: this describes a small triangular density at the highest point of the hemidiaphragm dome with upper lobe (± middle lobe) collapse – this is a useful ancillary sign
 ‘Shifting granuloma’ sign: a change in position of a granuloma with hyperexpansion
‘Shifting granuloma’ sign: a change in position of a granuloma with hyperexpansion
 An elevated hemidiaphragm (particularly with left upper lobe collapse) is of limited value
An elevated hemidiaphragm (particularly with left upper lobe collapse) is of limited value
COMPUTED TOMOGRAPHY OF LOBAR COLLAPSE
 However this can also be caused by excessive mucus production combined with decreased mucociliary function (e.g. ABPA, asthma, cystic fibrosis)
However this can also be caused by excessive mucus production combined with decreased mucociliary function (e.g. ABPA, asthma, cystic fibrosis)
 a proximal obstructing lesion may not cause complete lobar collapse (if a fissure is incomplete and allows collateral air drift)
a proximal obstructing lesion may not cause complete lobar collapse (if a fissure is incomplete and allows collateral air drift)  occasionally the parenchyma and airways can become fluid filled due to a central obstructing lesion with little or no volume loss giving rise to the appearance of a ‘drowned lobe’
occasionally the parenchyma and airways can become fluid filled due to a central obstructing lesion with little or no volume loss giving rise to the appearance of a ‘drowned lobe’  false-positive diagnoses may be due to bronchial strictures, mucous plugs, or compression by a large pleural effusion
false-positive diagnoses may be due to bronchial strictures, mucous plugs, or compression by a large pleural effusion
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Pulmonary lobar collapse
 broncholiths
broncholiths  focal bronchostenosis due to inflammation or trauma
focal bronchostenosis due to inflammation or trauma
 tumours are very rare
tumours are very rare

 the ipsilateral main bronchus becomes more vertically orientated
the ipsilateral main bronchus becomes more vertically orientated
 little mediastinal shift is seen with an acute upper lobe collapse but there is a greater shift with chronic fibrotic upper lobe volume loss
little mediastinal shift is seen with an acute upper lobe collapse but there is a greater shift with chronic fibrotic upper lobe volume loss
 it is commonly seen in the right upper lobe (but can be seen in any lobe)
it is commonly seen in the right upper lobe (but can be seen in any lobe)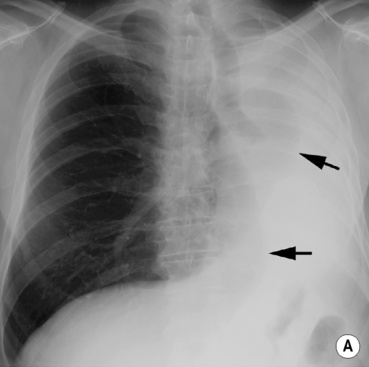
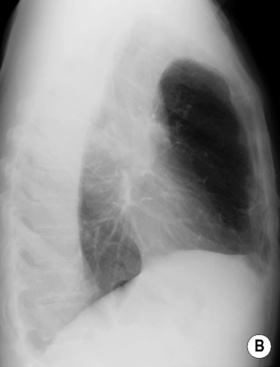
 the endobronchial component is visible as an abrupt cut-off of the left main bronchus. Note the marked displacement of the right lung anteriorly and posteriorly across the midline (arrows). Note the marked anterior hyperlucency of the thorax on the lateral view (B).*
the endobronchial component is visible as an abrupt cut-off of the left main bronchus. Note the marked displacement of the right lung anteriorly and posteriorly across the midline (arrows). Note the marked anterior hyperlucency of the thorax on the lateral view (B).*





