Pseudofracture |
False appearance of midshaft fracture due to rotation or projection, especially in children. |
A vascular channel in the bone may simulate a fracture. |
Conoid tubercle |
Bump on posteroinferior distal one-third of clavicle. |
Attachment for the conoid portion of the coracoclavicular ligament. Ligament between conoid tubercle and coracoid process may undergo ossification, usually secondary to trauma. |
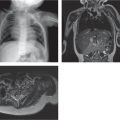
Posttraumatic osteolysis
Fig. 5.10
Fig. 5.11a, b |
Resorption of the distal or proximal ends of the clavicle. Acromioclavicular (AC) joint appears widened with erosions at the distal end. |
May follow 6–8 wk after trauma at the AC joint. |
Osteomyelitis |
Destruction and periosteal reaction. |
Primary infection of bone (spread from trauma or blood) or secondary spread from sterno-clavicular or AC joints. |
Hyperparathyroidism |
Generalized bone demineralization, erosion of the distal ends of the clavicles, and bone resorption along the inferior border of the distal clavicle at the attachment of the coracoclavicular ligament. |
Brown tumor may be seen in primary hyper-parathyroidism (see Table 5.75 ). Pseudofractures (Looser zones). |
Osteonecrosis |
Aseptic necrosis of the medial end of the clavicle (Friedrich disease). |
Sclerosis of the medial end of the clavicle may persist. |
Juvenile idiopathic arthritis (JIA) |
Erosions at the ends of the clavicles with widening of AC joint. |
Sternoclavicular joint involvement may be diff cult to appreciate on radiographs and may require cross-sectional imaging for detection of inflammatory changes. |
Ankylosing spondylitis |
Enthesopathy at the coracoclavicular and costoclavicular ligaments with bone proliferation and ligamentous calcification on radiographs and bone marrow edema on MRI. |
|
Tumor
Fig. 5.12 |
|
Langerhans cell histiocytosis, aneurismal bone cyst, hemangioma. Clavicle is rare site of involvement for fibrous dysplasia, metastasis, osteosarcoma, Ewing sarcoma, leukemia, and lymphoma. |
Radiation necrosis |
Spectrum of findings from localized bone demineralization to frank bone destruction. |
An osteochondroma may arise at the medial end of the clavicle following irradiation of the bone during childhood. Pathologic fractures often fail to heal (pseudarthrosis). Secondary osteosarcoma may develop as a late complication. |
Neurofibromatosis |
Pressure erosions. Tapering of the clavicle (“pencil pointing,” distal > proximal). |
|
Infantile cortical hyperostosis (Caffey disease) |
Cortical hyperostosis. Clavicle appears thick and wide and is surrounded by exuberant periosteal reaction. |
Infants less than 5 mo of age. Clavicles, ribs, and mandible are most common sites. DD: vitamin A toxicity. |
CRMO |
Bone destruction, extensive sclerosis, and bone enlargement. |
(see Table 5.1 ) |
Melorheostosis |
Marked cortical thickening and characteristic dripping candle wax appearance. |
Localized painful swelling and growth disturbances. Follows distribution of dermatomes. |