Short ribs do not extend as far anteriorly as the sternum; they lead to a decreased chest volume that may cause respiratory insufficiency. The more widely know dysplasias and syndromes with short ribs as a feature are discussed in Tables 5.3through 5.10.
Table 5.3 Ribs: short ribs
Diagnosis
Findings
Comments
Achondroplasia
Short and wide ribs with concavity at the rib end.
Narrowing of the intrapedicular distance (as apposed to normal widening) from L1 to L5 on AP projection. Rhizomelic shortening of the humeri, macrocephaly, depression of the nasion, scalloping of the posterior aspects of the vertebral bodies, square iliac bones, and a champagne glass–shaped pelvic inlet. DD: hypochondroplasia.
Thanatophoric dysplasia
Very short ribs that do not extend beyond the anterior axillary line.
Most common form of skeletal dysplasia that is lethal in the neonatal period. “H-” or “U-”shaped vertebral bodies, short and curved humeri, cloverleaf skull deformity, polydactyly, and hypoplastic iliac bones. DD: thanatophoric variants, asphyxiating thoracic dysplasia, homozygous achondroplasia, and achondrogenesis.
Short ribs with a horizontal course. The chest diameter is smaller in comparison to the abdomen.
Long bones are shortened, the iliac wings are small, and the acetabula may have spurs. The proximal humeral and femoral epiphyses may be ossified at birth. ± polydactyly. Adults have a high prevalence of medullary cystic renal disease. DD: Ellis-van Creveld dysplasia.
Small chest accentuates the size of the cardiomegaly.
Congenital heart disease (atrial septal defects) with cardiomegaly. Severe respiratory insufficiency results in high neonatal mortality (~50%). High prevalence among the Amish. Appearance of pelvis is similar to Jeune dysplasia. DD: Jeune dysplasia and short rib–polydactyly syndromes.
Other dysplasias and syndromes
For example, atelosteogenesis, Barnes syndrome, campomelic dysplasia, metatropic dysplasia, otopalatodigital syndrome, Schneckenbecken dysplasia.
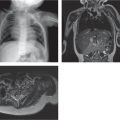
Fig. 5.2 Asphyxiating thoracic dysplasia. Jeune syndrome. Short ribs and scoliosis.Fig. 5.3 Chondroectodermal dysplasia. Ellis-van Creveld syndrome with a narrow chest, small iliac bones, and iliac spurs.
Table 5.4 Ribs: slender ribs
Diagnosis
Findings
Comments
Trisomies 8, 13, 18, and 21
Hypoplastic and thin ribs. 11 rib pairs.
In trisomy 18, a short sternum produces a shield deformity of the chest. Acute iliac angle is diagnostic. Ulnar deviation and flexion deformity of the fingers with curled thumb grasped by the fingers.
Neurofibromatosis
Slender, twisted, and/or deformed ribs that may be separated by neurofibromas.
For example, achondrogenesis, campomelic dysplasia, progeria, and Cockayne, Gorlin, Larsen, and Turner syndromes.
Table 5.5 Ribs: wide ribs
Diagnosis
Findings
Comments
Thalassemia major
Undertubulated and broad ribs with heterogeneous ossification.
The rib findings as well as widened dipole, hypoplasia of paranasal sinuses, paraspinal extramedullary foci, and hepatospleno megaly are rarely seen with aggressive marrow replacement and chelation therapy. DD: other chronic anemias, storage disease, and fibrous dysplasia.
Fibrous dysplasia
Affected ribs are widened.
Sickle cell anemia and thalassemia
Mucopolysaccharidosis
Ribs are thin proximally near the costovertebral junction and then wider distally.
External flaring of the iliac bones, vertebral body flattening and beaking, atlantoaxial instability, and brachydactyly. DD: Gaucher and Niemann-Pick diseases.
Gorlin (basal cell nevus) syndrome
Bifid, fused, or markedly splayed ribs.
Sprengel and pectus deformities, syndactyly, calcified falx cerebri, flame-shaped lucencies of the hands and feet. Radiologic findings contribute to the list of clinical criteria used to diagnose the syndrome.
Other dysplasias and syndromes
For example, achondroplasia, Erdheim-Chester disease, Niemann-Pick disease, osteopetrosis, pacman dysplasia, tuberous sclerosis.
Table 5.6 Ribs: miscellaneous rib anomalies
Diagnosis
Findings
Comments
Cervical ribs
Unilateral or bilateral, arise from the seventh cervical vertebra, and resemble hypoplastic first thoracic ribs.
Incidental finding (0.2% to 8% prevalence) or are associated with Klippel-Feil anomaly. Can compress adjacent nerves supplying the brachial plexus and vessels (thoracic outlet syndrome or aneurysm formation).
Eleven paired ribs
Occurs in 5%–8% of normal individuals and in one-third of patients with trisomy 21. Associated with several skeletal dysplasias including cleidocranial and campomelic dysplasia.
Pectus excavatum
Posterior ribs are horizontal, whereas the anterior ribs have a more vertical course.
A portion of the rib splits into two separate ribs.
May be incidental and discovered as a palpable mass. DD: Gorlin (or basal cell nevus) syndrome (fourth rib most commonly bifid).
Supernumerary ribs
Trisomy 21 syndrome (although 11 paired ribs is more common) and with VATER (vertebral defects, anal atresia, tracheoesophageal fistula with esophageal atresia, radial or renal dysplasia, and limb anomalies) association. Rarely seen as a variation of normal.
Concave notches found on the inferior rib surface.
Most commonly found as a variation of normal anatomy. Pressure erosion (saucerization) from enlarged vascular or neural structures. Notching associated with aortic coarctation usually affects ribs 4–8 (costal arteries are enlarged above the aortic stenosis) and is rare before the age of 8 y. DD: coarctation of the aorta, neurofibromatosis, thalassemia, and postoperative Blalock-Taussig shunt (right-sided notching).
Cerebrocostomandibular syndrome
Ribs have abnormal costovertebral articulations and posterior ossification gaps that resemble fractures.
Gaps will eventually ossify. Usually 11 pairs of ribs. Microcephaly, micrognathia, and congenital heart disease. DD: multiple rib fractures.
Fig. 5.4a, b Rickets with cupping at the rib ends (arrows in a) and metaphyses about the knee (b).Fig. 5.5 Rib notching. Coarctation of the aorta. Rib notching (arrowheads) and the figure-three sign (arrow).
Table 5.7 Ribs: expansile rib deformity
Diagnosis
Findings
Comments
Fibrous dysplasia
Expansile mixed lucent and sclerotic non-aggressive lesion with a ground-glass matrix, cortical thinning, and modeling deformity.
Most common cause of a benign expansile rib lesion. DD: simple bone cyst, enchondroma, and brown tumor of hyperparathyroidism.
Skeletal survey may be useful to detect multiple lesions.
Lymphangiomatosis (Gorham disease)
Well-defined areas of lucency that may coalesce and replace large portions of bone. Osteolytic with a thin sclerotic rim. Osteolysis may be massive.
Thought to be due to malformation/proliferation of lymphatic vessels in bone.
Fig. 5.6 Malignant tumors. Rib expansion and destruction from metastatic rhabdomyosarcoma (arrow).Fig. 5.7 Malignant tumors. Chest wall mass with rib destruction from Ewing sarcoma.Fig. 5.8 Langerhans cell histiocytosis. Lucent and expansile rib lesion produced by Langerhans cell histiocytosis (arrows).