CHAPTER 21 Clinical Single Photon Emission Computed Tomography Cardiac Protocols
Nuclear medicine has become a remarkable diagnostic tool to identify and to stratify patients with suspected coronary artery disease (CAD) with pivotal prognostic implications. Myocardial perfusion imaging (MPI) provides an accurate measurement of coronary narrowing leading to inducible perfusion abnormalities with prognostic implications (Fig. 21-1). The relationship between the degree of coronary stenosis and the maximal hyperemic response was first reported more than 30 years ago.1 Myocardial regions with relatively decreased post-stress radiotracer uptake and resting normalization indicate a misbalance between oxygen supply and myocardial demands, characteristic of ischemia. Nonreversible myocardial perfusion defects normally relate to necrosis or infarction. Current imaging protocols allow the accurate assessment of relative regional perfusion and myocardial function at rest and stress based on regional blood flow heterogeneity. Gated single photon emission computed tomography (SPECT) represents nearly 95% of all procedures performed today in cardiac nuclear medicine. This chapter reviews the different imaging SPECT acquisition protocols that are currently in use as well as the principal indications.
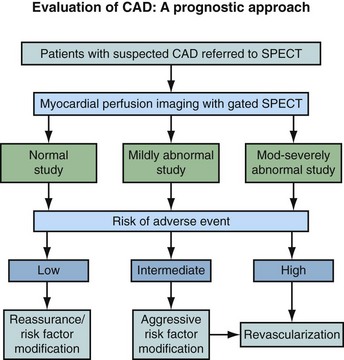
 FIGURE 21-1
FIGURE 21-1TECHNICAL REQUIREMENTS
201Tl Imaging Protocols
During the last two decades, thallium 201 (201Tl) has been used as a myocardial perfusion tracer. After an intravenous injection, the initial myocyte uptake is mainly determined by regional myocardial perfusion, whereas the integrity of the cell membrane is predominantly important for delayed imaging of tracer retention (potassium ion total distribution). Regional thallium activity on delayed images acquired early (3 to 4 hours) or late (8 to 72 hours) after stress has been used to demonstrate the presence and extent of viable myocardium based on the phenomenon termed thallium redistribution.2 Intracellular thallium uptake through the sarcolemmal membrane is maintained during long periods if regional myocardial blood flow is sufficiently preserved to be able to deliver the isotope to the myocytes. Redistribution is thought to represent areas of ischemic but viable myocardium, whereas fixed, non-redistributing defects are thought to represent nonviable, fibrotic scar.
When 201Tl alone is used, a variety of different acquisition protocols of stress imaging have been employed, including redistribution and reinjection imaging. Although different 201Tl imaging protocols have been employed, stress-redistribution-reinjection and rest-redistribution SPECT imaging protocols are the most currently used to assess myocardial viability.3 Reinjection of 1 mCi of 201Tl after 3 to 4 hours of redistribution imaging detects viable tissue in 35% to 49% of segments with fixed irreversible 201Tl defects with conventional stress-redistribution protocols.4 An inverse relationship has been reported between regional thallium activity in irreversible defects and the amount of myocardial fibrosis.5 Perrone-Filardi and colleagues6 demonstrated the nearly linear relation between thallium activity and the likelihood of recovery of regional function after revascularization. Overall sensitivity of several stress-redistribution-reinjection studies averaged 85% with a lower specificity (averaging 47%), suggesting that this protocol tends to overestimate the potential for contractile function recovery.2
Rest-redistribution 201Tl imaging is a valid alternative to discriminate viable from nonviable myocardium when the clinical question is to identify viability and not inducible ischemia.7,8 Studies have reported that 24-hour imaging after rest injection detects additional areas of viable myocardium compared with 4-hour imaging alone, possibly related to higher resting blood flow levels.9
Tc 99m Labeled Imaging Protocols
One-Day Protocol
Regarding viability assessment, earlier studies using primarily planar scintigraphy and visual interpretation suggested that Tc 99m sestamibi underestimates myocardial viability in chronic CAD and left ventricular dysfunction. Dilsizian and colleagues10 described the utility of quantitative Tc 99m sestamibi imaging when the severity of decrease in Tc 99m sestamibi uptake within irreversible defects was considered or when an additional redistribution image was acquired after the rest injection for detection of dysfunctional but viable myocardium. A significant inverse linear relationship has been described between Tc 99m sestamibi uptake and myocardial fibrosis in biopsy specimens.11 Several approaches have been introduced to increase the diagnostic performance of Tc 99m sestamibi for the identification of viable myocardium, such as functional evaluation of the left ventricle by first-pass radionuclide ventriculography, gated SPECT acquisition perfusion images,12 and intravenous administration of nitrates to reduce resting hypoperfusion and to increase the correspondence of the resting images with myocardial viability.13
Fatty acid analogues marked with iodine isotopes (123I, 131I) have been employed to study myocardial metabolism on the basis of the principle that in a viable but ischemic myocardium, fatty acids are mainly esterified and incorporated into the triglyceride and phospholipid blood pool and are slowly metabolized, with subsequent clearance rate reduction.14 Early data suggested that this method may provide data comparable to 201Tl protocols in patients with left ventricular dysfunction or after an acute myocardial infarction. These tracers may prove to be of more value in the near future, considering the key role that oxidative metabolism plays in preservation of myocardial function.
Dual-Isotope Protocols
Dual-isotope imaging protocols using Tc 99m labeled compounds and 201Tl are based on the ability of the Anger camera to collect data from the two different energy windows representing each radiotracer. Simultaneous and separate dual-isotope imaging protocols have been described.15,16 Two of the major advantages of these protocols are the possibility of shortening the duration of a complete stress or rest redistribution protocol and the superior capability of 201Tl to assess myocardial viability. Separate acquisition times can reduce the necessity of downscatter correction that can diminish 201Tl contrast images, leading to an overestimation of defect reversibility; this can be achieved by acquiring 201Tl data sets before the administration of Tc 99m because of the very limited (2.2%) contribution of 201Tl into the Tc 99m energy window.
Gated SPECT
Most of the current imaging protocols perform a simultaneous ECG gating during at least the stress data set acquisition.17 Gated SPECT can be performed with 201Tl or Tc 99m compounds. One of the major advantages is the possibility of measuring contractile function and the left ventricular ejection fraction.
STRESS PROTOCOLS
Exercise Testing
This is the most common form of stress during MPI. Exercise testing is performed on the treadmill according to the Bruce protocols and allows the assessment of different hemodynamic variables, such as exercise capacity, blood pressure, and heart rate responses. It is imperative that the intravenous injection of the radiotracer be performed at maximal stress and that exercise continue for at least an additional 60 seconds to ensure optimal myocardial concentration. The traditional goal of the test as an acceptable level of cardiac workload has been the achievement of at least 85% of the maximum predicted heart rate (220 − age). Prognostic information from the exercise test should be integrated with MPI because the patients with mild to moderate perfusion defects who achieved a heart rate higher than 80% had a very low risk for major cardiac events and cardiac death.18 At the same time, patients with a reported normal MPI study but abnormal heart rate reserve were at the same risk for suffering a major cardiac event as those with normal heart rate reserve achieved and abnormal MPI studies (Tables 21-1 and 21-2). A maximal stress test may satisfy diagnostic purposes if it goes beyond the hemodynamic threshold of triggering the ischemic symptoms. However, it may not reveal the full amount of jeopardized myocardium and may be inadequate for the evaluation of cardiac risk in a patient scheduled to have major noncardiac surgery. A submaximal exercise test (not achieving 85% of the targeted heart rate) may still be a valid alternative for evaluation of ischemic risks after cardiac events. To achieve the most adequate level of cardiac stress and to avoid suboptimal stress testing, patients should discontinue antianginal medications (β blockers and calcium blockers for 36 to 48 hours and long-acting nitrates for 12 hours).19 Furthermore, all patients should be studied in the fasting state, having been in a nothing-by-mouth status for at least 4 hours before the study, regardless of the stress method to be employed. All caffeine, including beverages and chocolate, especially before pharmacologic stress testing, should be avoided for at least 24 to 48 hours to avoid block of the endothelial receptors and their dilatory effect.
| Bicycle or treadmill |
| Maximal exercise and at least 85% of age-predicted maximum heart rate |
| Monitor ECG continuously (9 or 12 leads) |
| Blood pressure recorded every 2 to 3 minutes |
| Tracer injection at peak exercise; keep exercising for at least 1 additional minute |
| Assess electrical changes or symptoms |
TABLE 21-2 Exercise Stress Contraindications
| Acute aortic dissection |
| Symptomatic aortic stenosis |
| Uncontrolled cardiac arrhythmias |



