(1)
Kaiser Permanente, Southern California Permanente Medical Group, Riverside, CA, USA
(2)
Molecular Imaging Center and PET Clinic, University of Southern California, Los Angeles, CA, USA
(3)
Department of Radiology, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA
Case 6.1: Ascending Colon Cancer
History
Patient is a 35-year-old female with ascending colon cancer for initial staging.
Findings
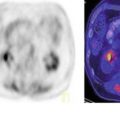
A soft tissue mass in the colonic hepatic flexure with SUV max 7.7 consistent with primary tumor (Fig. 6.1). There are focal areas of increased uptake which could represent mesenteric nodes and/or peritoneal/omental metastases. There are innumerable hypermetabolic panlobar metastases in the enlarged liver.

Fig. 6.1
Case 6.2: Mid-ascending Colon Cancer
History
49-year-old male newly diagnosed with adenocarcinoma of the ascending colon, with possible metastasis to the lung and liver.
Findings
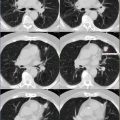
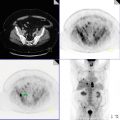
There are hypermetabolic metastatic lesions seen in the right hepatic lobe (involving segments 5, 6, and 7), with the most avid lesion seen in segment 6, demonstrating SUV max 9.4 (Fig. 6.2). There is an annular lesion in the mid-ascending colon, demonstrating SUV max 18.3, compatible with known site of primary neoplasm.

Fig. 6.2
Pearls and Pitfalls
Accurate preoperative staging is essential for the planning of optimal therapy considering the many therapeutic options available.
Discussion
CRC is the third most commonly diagnosed cancer in males and females. The survival rate depends on the stage at the time of diagnosis. Approximate 5-year survival rates are stage I 90 %, IIA 85 %, IIB 72 %, IIIA 83 %, IIIB 64 %, IIIC 44 %, and IV 8 %.
Case 6.3: Peritoneal Metastases from Colon Cancer
History
Patient with metastatic colorectal cancer has history of cholecystectomy. Patient had last chemotherapy in 2005. This scan is being done for suspected recurrence in 2011.
Findings
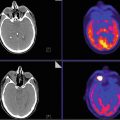
There is a peritoneal nodule with adjacent peritoneal thickening measuring 1.2 cm in the right false pelvis with SUV max 16.3 (Fig. 6.3). There is an intensely active lesion anterior to the capsule of the liver at the gallbladder fossa measuring 1.7 × 0.7 cm, with SUV max 7.3.

Fig. 6.3
Pearls and Pitfalls
1.
Roughly one in five patients with colorectal cancer develops peritoneal minimal residual disease after surgical resection.
2.
About one in seven patients develops peritoneal carcinomatosis.
Discussion
There is a vast body of research addressing hematogenous metastasis; little is known about the biology of peritoneal spread of colorectal cancer. The development of peritoneal carcinomatosis involves well-defined steps including cell shedding and transport, adhesion to the mesothelial layer, invasion of and proliferation into the submesothelial stroma, and potential access to the systemic circulation.
Case 6.4: Recurrent Adenocarcinoma of the Rectum Manifesting as Solitary Inguinal Adenopathy
History
Patient with moderately differentiated adenocarcinoma of the rectum diagnosed in 2005 status post resection with nodal and lung metastases. Patient underwent resection of the left upper lung lesion in April 2008. Patient is status post chemotherapy in April 2008 and radiation therapy in August 2005. No interval treatment. Scan being done for restaging.
Findings
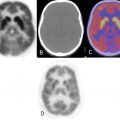
A new 2 × 2.3 cm left inguinal nodal mass with SUV max 12.8 is consistent with recurrent metastatic disease (Fig. 6.4).

Fig. 6.4
Pearls and Pitfalls
Low rectal carcinoma is more likely to present with pulmonary, osseous, and ilioinguinal metastases because of hemorrhoidal venous circulation.
Discussion
The usual pattern of regional lymph node metastasis in colorectal carcinoma follows the vascular distribution in the mesocolon. Tumors originating from the cecum spread to the ileocolic nodes, whereas tumors of the ascending and the proximal transverse colon drain in lymph nodes of the right colic and middle colic arteries reaching the superior mesenteric artery lymph nodes. Tumors originating from the descending colon spread to the left colic artery nodes, whereas those of the sigmoid colon reach the sigmoid artery nodes ending in the inferior mesenteric artery lymph nodes. Both the inferior and the superior mesenteric artery nodes belong to the preaortic nodes. Tumors in the rectum can spread by two different routes. The lymphatic drainage of tumors of the upper rectum reaches the inferior mesenteric artery lymph nodes via the superior rectal arteries. Metastases of tumors originating from the lower rectum reach the internal iliac nodes by following the pathway of the middle and the inferior rectal arteries and then the common iliac and the para-aortic nodes. Tumors of the anal region spread to the superficial inguinal lymph nodes ascending along the femoral vessels to the deep inguinal nodes and along the iliac vessels to the para-aortic nodes. After radical surgery for carcinoma of the rectum with interruption of the normal pathway of lymphatic drainage, recurrent disease may find an alternative retrograde route to the superficial and deep inguinal nodes.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


