Anomalies of form
Lacuna magna
Posterior urethral valve
Anterior urethral valve
Congenital stenosis
Congenital diverticulum
Congenital anterior diverticulum
Cowper duct dilatation (syringocele)
Prostatic utricle
Congenital polyps
Megalourethra
Congenital fistula
Anomalies of number
Duplication
Urethral groove malformations
Epispadias
Hypospadias
Anomalies of Form
Lacuna Magna (Sinus of Guérin)
The most common and asymptomatic urethral anomaly is diverticular dilatation of the roof of the fossa navicularis, which develops due to incomplete fusion of the glandular urethra and ectoderm at the tip of the penis.
Lacuna magna is a very common anomaly which may also be regarded as a normal variation since it is seen in up to 30 % of boys.
Posterior Urethral Valves
Posterior urethral valves are the commonest cause of congenital urethral obstruction, with an incidence of 1 in 5,000–8,000 of live male births.
Various types occur, the commonest of which are a bivalvular form and a diaphragm with a central pinhole. Posterior urethral valves can cause marked or even life-threatening bladder outlet obstruction, with upper tract deterioration.
Anterior Urethral Valves
Anterior urethral valve is a rare congenital anomaly of unclear embryological origin, involving anterior urethra.
Anterior urethral valves are seven to eight times less frequent than posterior counterparts.
Congenital Stenosis
Congenital stenosis of the urethra comprises narrowing of the urethral lumen of developmental origin. It may be seen at any level of the urethra, most commonly at the junction of anterior and posterior urethra.
Congenital Urethral Diverticula
Congenital diverticula include anterior diverticulum, Cowper duct dilatation (syringocele), and prostatic utricle cyst.
Anterior diverticulum develops on the ventral surface of the penile urethra as a result of either focal incomplete development of the corpus spongiosum or incomplete fusion of a segment of the urethral plate.
Dilatation of Cowper duct, which drains into the membranous urethra, may appear as a urethral diverticulum.
The prostatic utricle is not a Müllerian duct remnant; it has recently been shown that the utricle forms as an ingrowth of specialized cells from the dorsal wall of the urogenital sinus as the caudal Müllerian ducts regress. Its size usually diminishes in the ninth week, but in some cases of hypospadias and intersexuality, a deep utricle is found; its size is generally inversely proportional to the degree of hypospadias. Cystic dilatation of the utricle may occur, and in some cases of this entity, there is a direct connection between the cavity of the utricle and the urethra; absence of such a communication results in a prostatic utricular cyst.
Megalourethra
Megalourethra is a congenitally enlarged urethra, which may be scaphoid or fusiform in type. The scaphoid results from a developmental anomaly of the corpus spongiosum. In the fusiform type, the corpora cavernosa are also affected.
Megalourethra is associated with Prune Belly and VATER syndromes.
Congenital Fistula
Congenital fistula occurs in neonates with imperforate anus. Boys with high imperforate anus frequently have a connection of rectum with the lower urinary tract, usually at the level of the prostatic urethra and, rarely, at the level of the bladder.
Congenital stenosis, congenital diverticula, and megalourethra are extremely rare anomalies.
Anomalies of Number
Urethral duplication may be incomplete or complete with one or two orifices.
Incidence and prevalence of urethral duplication is extremely rare.
Urethral Groove Malformations
Hypospadias
It is an abnormally located opening of the urethral meatus anywhere along the ventral aspect of the penis from the glans to the perineum.
Hypospadias is a relatively common anomaly, occurring in 0.3–0.8 % of male births.
Epispadias
It is a congenital defect in dorsal urethra, mostly seen as an element of the epispadias-bladder exstrophy complex.
Epispadias-bladder exstrophy complex occurs in 1 of 33,000–40,000 in live births; sporadic epispadias is extremely rare.
Normal Anatomic Variations of the Urethra
Male Urethra
A ring-like narrowing can be seen in the proximal bulbar urethra that is believed to be caused by a normal tendinous sling of the bulbocavernous muscle. This narrowing is called by urologists as “Cobb’s collar.”
Female Urethra
Spinning Top Urethra
On voiding, the female urethra may appear ovoid, tubular, funnel-, or carrot-shaped; most of these variations are considered normal (Fig. 13.1).
Fig. 13.1
Spinning top urethra. Axial (a), coronal reformatted (b), and sagittal reformatted (c) images demonstrate dilatation of proximal urethra with spinning top shape (arrows) in a 19-year-old female (B bladder)
“Spinning top” appearance of the urethra represents a widely distended proximal urethra; it is often considered normal but may be associated with bladder instability in up to 57 % of patients.
Since this finding was frequently associated with vesicoureteral reflux (VUR) and urinary tract infections, it was attributed to a distal obstruction which caused increased pressure and dilatation of the proximal portion of the urethra.
With the assumption that distal urethral obstruction was present, treatment in previous years often included urethral dilatation. When VUR was found not to be due to a distal obstruction, but instead due to an abnormal configuration of the vesicoureteral junction which resolved spontaneously with age, urethral dilatation was discontinued. Spinning top urethra was then considered a normal variant.
It was not until relatively recently, with the use of combined synchronous video and pressure recordings, that a spinning top urethra was reported to be a significant abnormality, usually indicating bladder instability. The proposed mechanism was that involuntary detrusor contractions produce dilatation of the posterior urethra as leakage is prevented with distal sphincter contraction. In patients with intrinsic weakening of the bladder neck, such as in a congenital wide bladder neck anomaly, this dilatation will be even more evident.
Treatment options for voiding dysfunction such as bladder instability include timed voiding, treatment of constipation, and prophylactic antibiotics for urinary tract infections. In some cases, anticholinergic medications, such as oxybutynin and propantheline, have been prescribed.
Imaging
Plain Film Radiography
Conventional X-rays have a limited role in the diagnosis of urethral anomalies.
Pubic diastasis is seen in epispadias-bladder exstrophy complex.
Retrograde Urethrography, Voiding Cystourethrography
Any obstructive lesion of the urethra causes dilatation of the normal urethra proximal to the lesion.
Long-standing obstruction of any cause in the urethra results in typical changes in the bladder as increased trabeculation and pseudodiverticular thickening of the bladder wall. Hydronephrosis or end-stage renal disease may ensue. Posterior urethral valves may occasionally be visualized as linear radiolucent bands in the posterior urethra (Figs. 13.2 and 13.3). Dilatation, elongation, or deformation of the urethra proximal to the valves and obstruction findings in the bladder and upper urinary tracts may be observed.
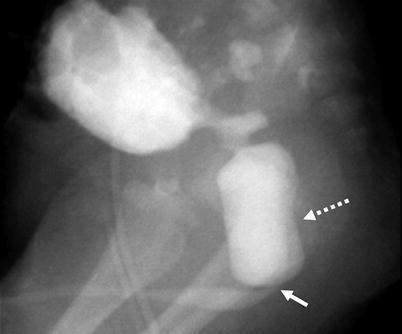
Fig. 13.2
Cystogram of the bladder. Posterior urethral valve (arrow) and dilated posterior urethra (dotted arrow)
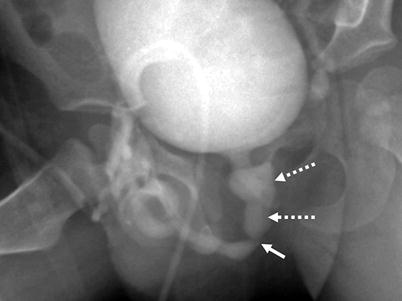
Fig. 13.3
Posterior urethral valve. A transverse luminal filling defect (arrow) and dilated posterior urethra (dotted arrows)
Anterior urethral valves may occasionally be visualized. Dilatation of the urethra to the level of the bulbar urethra (40 %), penoscrotal junction (30 %), or pendulous urethra (30 %) and obstruction findings in the bladder and upper urinary tracts may be evident.
Congenital stenosis of the urethra appears in cystography as eccentric or concentric narrowing of the lumen and obstruction findings in the bladder and upper urinary tract.
Congenital urethral diverticulum presents as a contrast-filled oval structure on the ventral aspect of the anterior urethra.
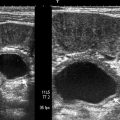
Cowper duct cyst (syringocele) is seen as an ovoid contrast filling at the ventral site of bulbous-pendulous urethra. Utricle cyst appears as a diverticular filling defect at the level of prostatic verumontanum (Fig. 13.4).
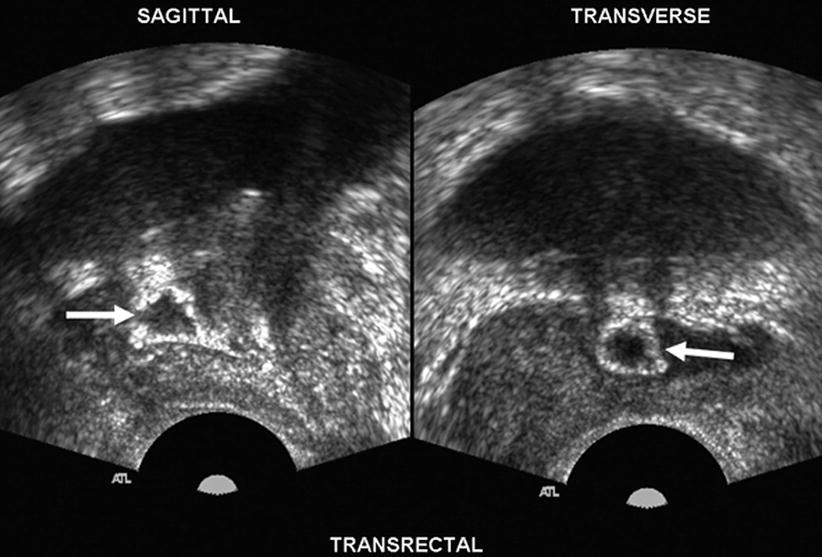
Fig. 13.4
Utricle cyst. Gray-scale transrectal ultrasound in sagittal and transverse planes demonstrates a midline utricle cyst with peripheral echogenic rim (arrows)
Megalourethra refers to very large urethra. It may be scaphoid (boat-like) or fusiform in shape.
Abnormal communication between the urethra and the rectum may be seen in congenital fistula.
Urethral duplication is seen as two opacified urethral lumens, either communicating or non-communicating (Fig. 13.5).

Fig. 13.5
Urethral duplication. Cystography reveals urethral duplication in a neonate
Ultrasound
Prenatal ultrasound may detect bilateral hydronephrosis and lack of optimum emptying of the bladder in subsequent exams on the same day in cases of posterior urethral valves. Dilatation of the proximal posterior urethra can be demonstrated. Oligohydramnios is an accompanying finding of severe obstruction secondary to urethral valves.
Posterior urethral dilatation to the level of the urethral valves can be shown by transperineal ultrasound exam which may also demonstrate bladder trabeculation, thickening of the bladder wall, and hydronephrosis.
Ultrasound is of limited usefulness in precise demonstration of anterior urethral valves, congenital stenosis, congenital diverticula, megalourethra, and urethral duplication. Findings of proximal obstruction may be demonstrated.
Magnetic Resonance Imaging
May be used in conjunction with retrograde urethrography to evaluate complex urinary system anomalies
Pathology
Posterior urethral valves are obstructive mucosal folds that are found infrequently in the region of the verumontanum; they are the commonest cause of congenital urethral obstruction.
Various morphologic forms of valves have been described, but they appear most commonly as a bivalvular structure or as a diaphragm with a central pinhole (Fig. 13.6).
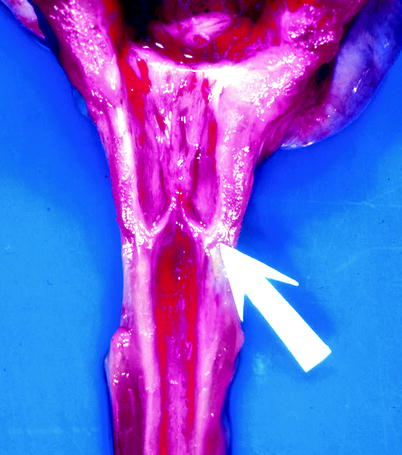
Fig. 13.6
Posterior urethral valves. The arrow indicates mucosal folds that appear to be based near the verumontanum (From MacLennan GT, Resnick MI, Bostwick DG. Pathology for urologists. Philadelphia: Saunders; 2003, with permission)
Posterior urethral valves in any form can cause significant or even life-threatening bladder outlet obstruction, with upper tract deterioration.
The obstructing folds consist of normal urothelium overlying stroma that has a variable degree of chronic inflammation and edema.
Treatment involves endoscopic ablation of the folds, and usually no tissue is submitted for histologic evaluation.
In bladder exstrophy, there is a defect in the infraumbilical portion of the anterior abdominal wall and ventral bladder wall, resulting in exposure of the posterior wall of the bladder (Fig. 13.7). At the level of the pubis, the pubic symphysis is absent and rectus abdominis muscles are divergent. Penile abnormalities include epispadias and bifid glans penis.

Fig. 13.7
Epispadias-bladder exstrophy complex. The bladder mucosa is exposed and edematous. The penis shows epispadias; the urethra is unformed (Photo courtesy of Jonathan Ross, M.D. and Katherine Hubert, M.D.)
Differential Diagnosis
Low-grade obstructing congenital stenosis or anterior urethral valves in older patients may not be difficult to distinguish from acquired stenosis (strictures).
False luminal tracts that develop secondary to periurethral inflammation may resemble urethral duplication (Fig. 13.8).
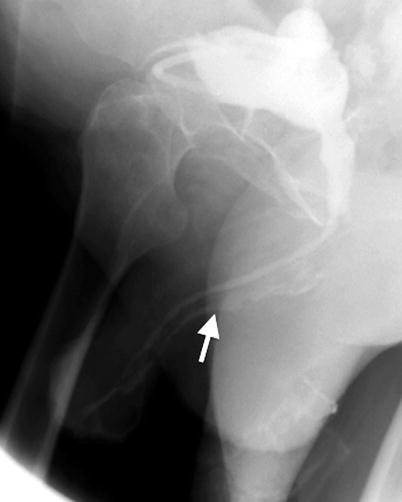
Fig. 13.8
False lumen mimicking urethral duplication. Cystogram demonstrates sinus tract (arrow) inside the corpus spongiosum secondary to inflammatory urethritis
Traumatic disruption of the urethra may form a periurethral cavity that may mimic a congenital urethral diverticulum. Whereas a diverticulum typically is smooth walled, a cavity of traumatic origin is more likely to an irregular outline (Fig. 13.9).
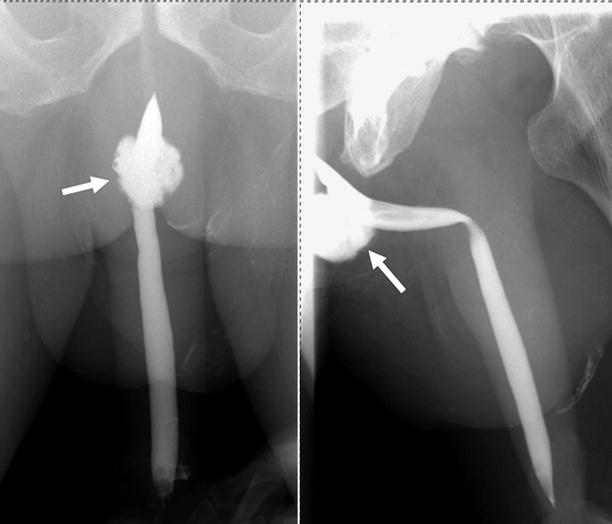
Fig. 13.9
Urethrospongiosal connection with pouch formation mimicking urethral diverticulum. Anteroposterior (a) and oblique (b) views of retrograde urethrogram demonstrate contrast filling on the ventral side of the penoscrotal junction (arrows). The patient had a history of straddle-type injury that resulted in traumatic pouch
Pearls and Pitfalls
During retrograde urethrography, the catheter should be placed as distal as possible, in order not to bypass obstructive lesions, such as posterior or anterior urethral valves, or congenital stenosis (Fig. 13.10).

Fig. 13.10
Improper cannulization of the urethra for evaluation of a congenital stenotic lesion. The catheter is in the bladder which passed through the posterior urethral valve (arrow)
Voiding cystourethrography exams should always be performed with the patient in an oblique or lateral position for better depiction of the obstructing lesions.
Perineal ultrasound should be performed in addition to routine ultrasound exams when obstructive congenital urethral lesions are suspected.
Acquired Nonneoplastic Disorders of the Urethra
Inflammatory Diseases
General Information
Inflammatory diseases of the urethra may be classified as infectious and noninfectious urethritis.
Infection-related urethral lesions include strictures related to gonorrhea or tuberculosis and condyloma acuminatum secondary to human papillomavirus infection.
Noninfectious inflammations include chemical urethritis (due to soap, cosmetics, spermicidal condom, etc.) and traumatic urethritis (repetitive self-catheterization, interventions, etc.).
The diagnosis of urethritis is made clinically and no imaging is necessary in uncomplicated cases.
Potential complications of urethritis include urethral stricture, periurethral abscess, and periurethral fistula.
Sexually transmitted infections resulting in urethritis are common.
Condyloma acuminatum involves the urethra in 0.5–5 % of male patients.
Tuberculosis of the urethra is rare.
The frequency of chemical and traumatic urethritis is difficult to estimate.
Imaging
Retrograde Urethrography