Congenital and Developmental Abnormalities of the Spine
Gaurav Jindal
Pamela H. Nguyen
Rafeeque Bhadelia
QUESTIONS
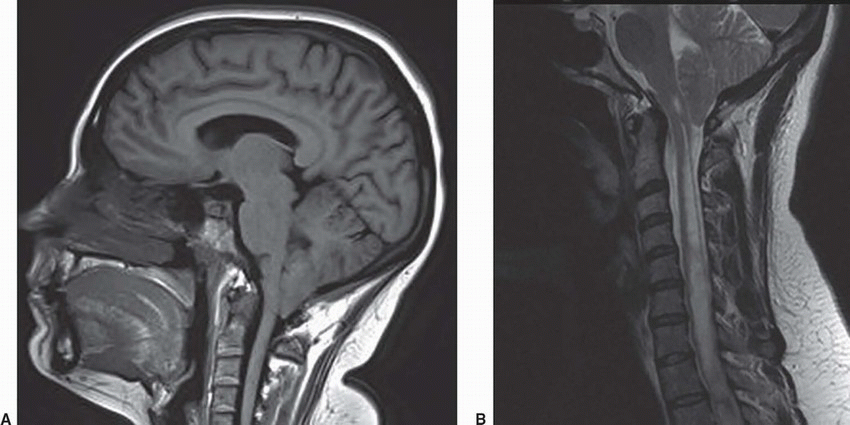
1 Patient A presents with cough-induced headaches. Patient B presents with upper extremity sensory deficits. MRI was performed for further assessment. Key images are shown below.
|
1a Which of the following is the most accurate diagnoses based on the images shown?
A. Both patients have Chiari 1 malformation.
B. Only patient A has Chiari 1.
C. Only patient B has Chiari 1.
D. Patient A has Chiari 1 and patient B has Chiari 2 malformation.
|
View Answer
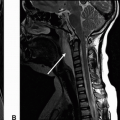
1a Answer A. Both patients have Chiari I malformation. Both patients have tonsillar ectopia with downward positioning of the cerebellar tonsils measuring at least 5 mm beyond the foramen magnum. There is an associated syrinx with patient B. These findings are compatible with Chiari 1 malformation.
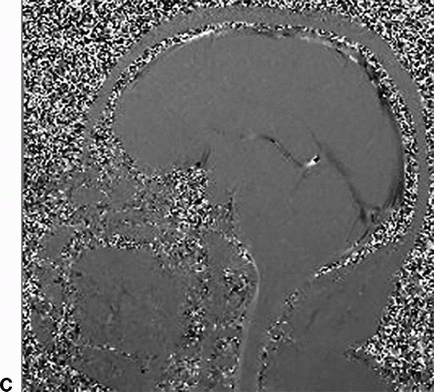
1b Additional advanced imaging was performed to understand the CSF flow dynamics, and the image is shown. Which of the following MR imaging sequences was used to obtain the image?
A. 3D steady-state gradient echo sequence such as CISS/FIESTA
B. Subtraction MR myelogram
C. Phase-contrast sequence CSF flow
D. 3D volumetric fast spin echo T1w
View Answer
1b Answer C. Phase-contrast sequence CSF flow. The image shown below (C) is a sagittal plane phase-contrast CSF flow sequence. The arrow points to the lack of flow-related signal in the dorsal subarachnoid CSF space at the cervicomedullary junction.
|
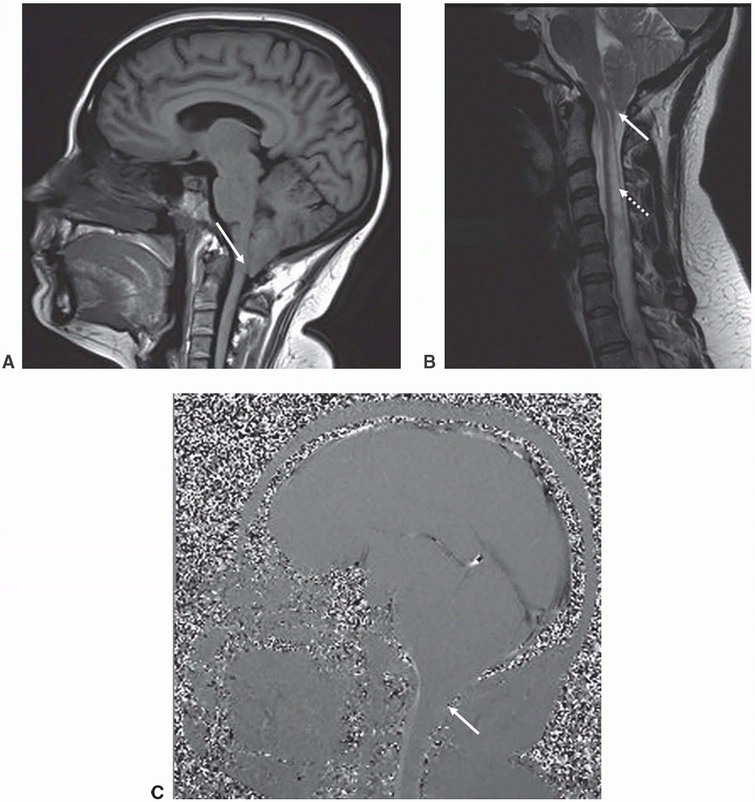
Imaging Findings: Sagittal T1w image in patient A and sagittal T2w image in patient B showing tonsillar ectopia (solid arrow A and B) with a syrinx seen in the upper cord in patient B (dotted arrow, B). Note lack of flow-related signal in the dorsal subarachnoid CSF space in phase-contrast CSF flow study in image C (solid arrow, C).
Discussion: Chiari 1 malformation.
Chiari 1 malformation is defined as inferior displacement of the cerebellar tonsils below the foramen magnum typically by at least 5 mm. It may be idiopathic or could be secondary to posterior fossa or craniovertebral junction anomalies. Caudally displaced tonsils are typically pointed or peg-like.
The most common complications of Chiari 1 result from altered CSF flow dynamics and include syringohydromyelia and hydrocephalus.
Chiari 1.5 is a more recently described entity, which combines features of Chiari 1 with inferior descent of the brainstem, typically the inferior margin of 4th ventricle (obex) lying below the foramen magnum.
Phase-contrast CSF flow imaging can be useful in evaluating CSF flow at the foramen magnum. Treatment in symptomatic patients most often consists of suboccipital craniectomy, and often also resection of the posterior arch of C1, with the goal to restore normal CSF flow.
References: Barkovich AJ. Congenital anomalies of the spine. In: Barkovich AJ, Raybaud C. (eds). Pediatric neuroimaging, 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2011.
Tubbs RS, Iskandar BJ, Bartolucci AA, et al. A critical analysis of the Chiari 1.5 malformation. J Neurosurg 2004;101(2 Suppl):179-183.
A. Lipoma of filum terminale
B. Lipomyelocele
C. Myelomeningocele
D. Lipomyelomeningocele
View Answer
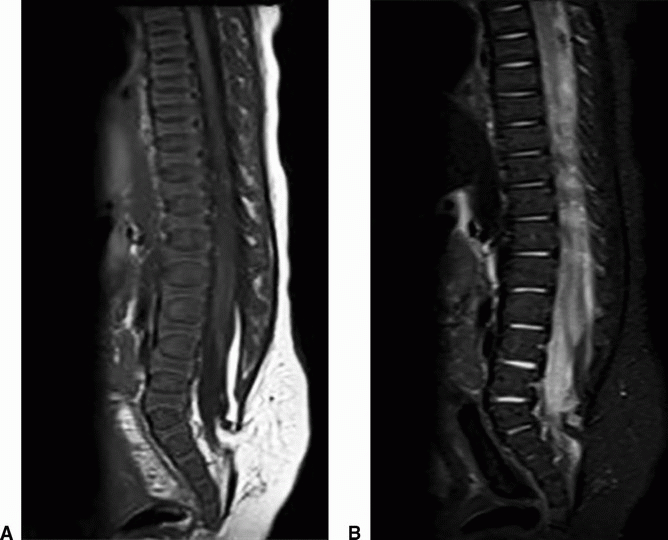
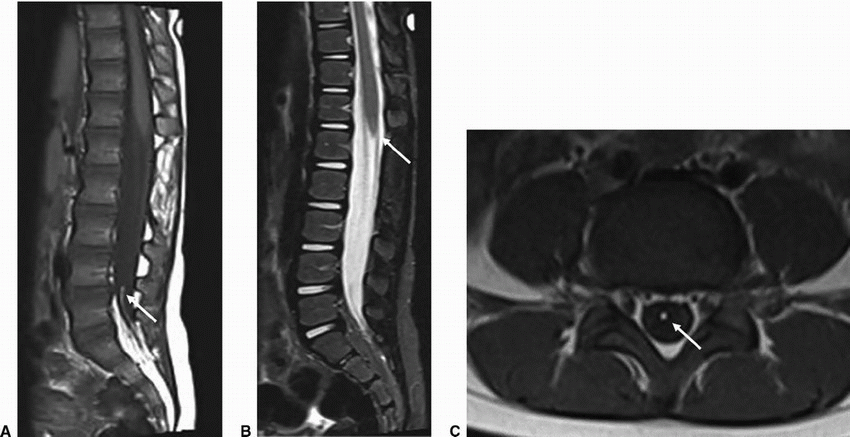
2a Answer B. Lipomyelocele. Sagittal T1 and STIR images show fat signal compatible with a lipoma, which is located between the neural placode ventrally and a spinal dysraphic defect dorsally. There is intact skin overlying the defect making the lesion most compatible with a lipomyelocele.
2b Which of the following is true about this entity?
A. Neural placode lipoma interface lies within the spinal canal.
B. Neural placode lipoma interface projects beyond the spinal canal.
C. Skin overlying the spinal dysraphic defect is disrupted.
D. Normally positioned conus medullaris
View Answer
2b Answer A. Neural placode lipoma interface lies within the spinal canal. Because of the above explained relationship of the structures involved, the interface lies within the spinal canal.
|
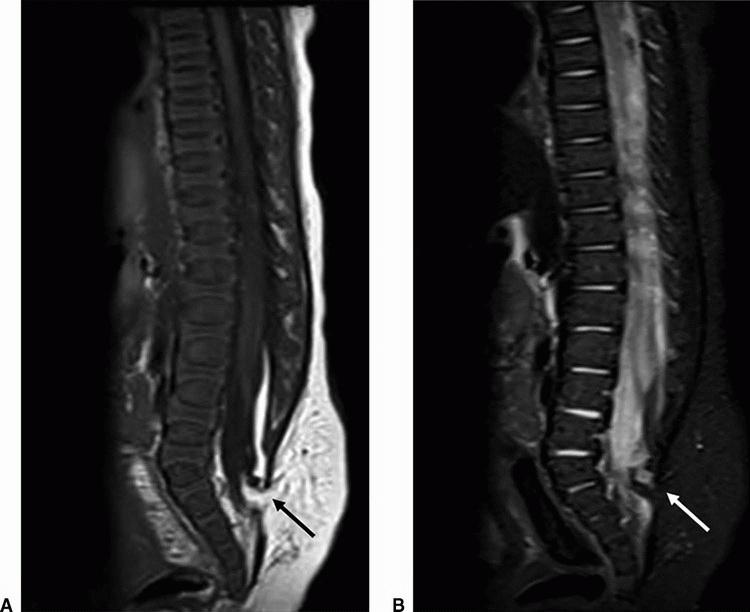
Imaging Findings: Sagittal T1w (A) and STIR (B) images show a tethered cord with a terminal syringomyelia. There is expansion of the lumbar spinal canal. There is fat containing signal compatible with a lipoma (black arrow) located between the neural placode ventrally and a sacral dysraphic defect dorsally with intact overlying skin (white arrow).
Discussion: Lipomyelocele.
Lipomyelocele refers to a skin-covered spinal dysraphism characterized by an intraspinal lipoma in contiguity with the subcutaneous fat via the dysraphic defect in the posterior elements. The neural placode is located within the spinal canal. If the neural placode projects through the dysraphic defect into the subcutaneous tissues, it is referred to as a lipomyelomeningocele. Location of the spinal lipoma may be intra- or extradural.
The cord is low lying and tethered to the intraspinal lipoma. There is typically mild expansion of the spinal canal and distention of the subarachnoid space at the level of lipomyelocele.
Differential Diagnosis: Imaging differentials include an intradural lipoma, which is characterized by an intact overlying dura and absence of communication with the subcutaneous fat. The spinal canal is not expanded although a tethered cord is often associated.
The other important differential is a myelomeningocele, which is an open spinal dysraphism where the neural placode projects outside the spinal canal and is not covered by the skin remaining exposed as a result to amniotic fluid in utero and air after birth.
References: Barkovich AJ. Congenital anomalies of the spine. In: Barkovich AJ, Raybaud C. (eds). Pediatric neuroimaging, 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2011.
Rufener SL, Ibrahim M, Raybaud CA, et al. Congenital spine and spinal cord malformations—pictorial review. AJR Am J Roentgenol 2010;194(3 Suppl):S26-S37.
3 Below are shown two contrasting developmental abnormalities in patients A and B. Key images from MRI are provided below.
|
3a Which of the following is the most likely diagnosis in patient A?
A. Type 1 caudal regression syndrome
B. Type 2 caudal regression syndrome
C. Tethered cord
D. Myelomeningocele
View Answer
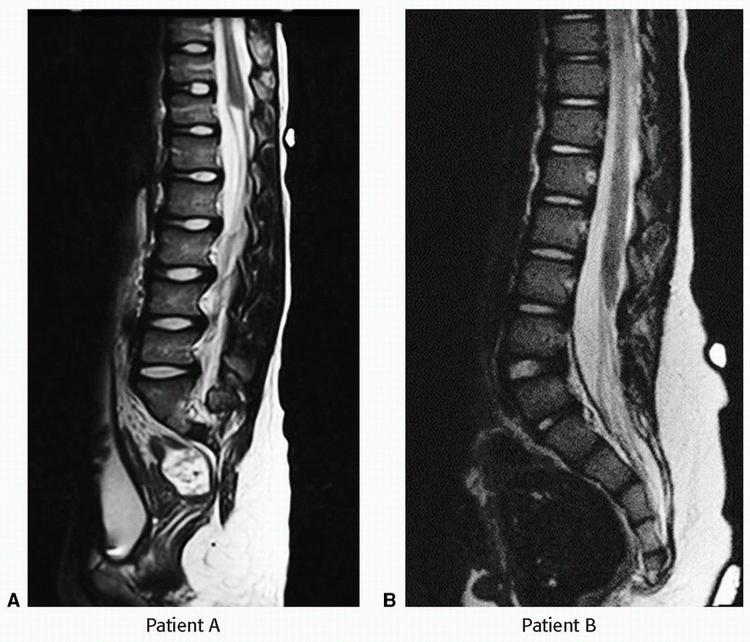
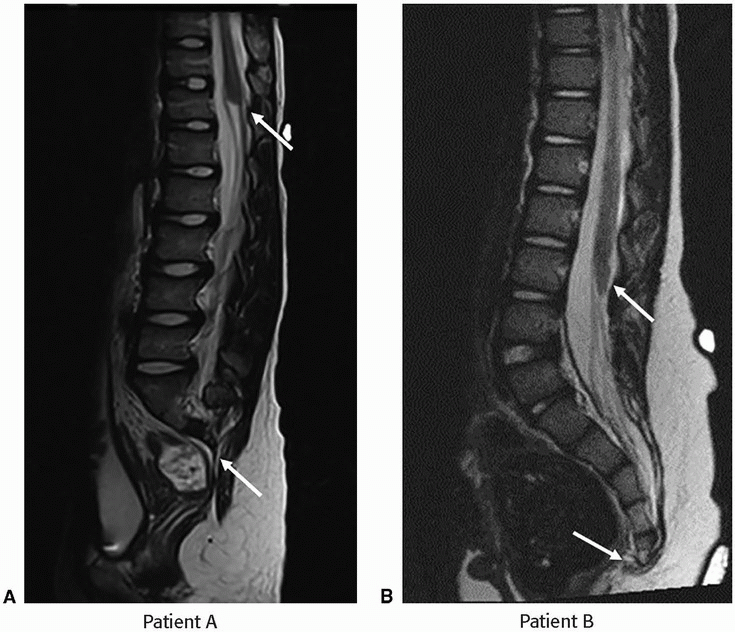
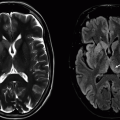
3a Answer A. Type 1 caudal regression syndrome. Sagittal T2-weighted image demonstrates sacral agenesis beyond S1. The conus medullaris terminates at T11-T12 and appears blunted.
3b Which of the following is the most likely diagnosis in patient B?
A. Type 1 caudal regression syndrome
B. Type 2 caudal regression syndrome
C. Tethered cord
D. Myelomeningocele
View Answer
3b Answer B. Type 2 caudal regression syndrome. Sagittal T2-weighted images demonstrate low-lying conus terminating at inferior border of L3. There is agenesis of the coccyx.
|
Discussion: Caudal regression syndrome.
Caudal regression syndrome is a complex congenital malformation characterized by varying degrees of lumbosacral agenesis/dysgenesis, along with malformations of the cord. Depending on the position of the conus, it is divided into two types:
Type 1: Abnormal high termination (above L1) of the conus, which is blunted or wedge shaped typically associated with sacral anomalies above S1.
Type 2: Low-lying tethered cord with less severe sacral agenesis, typically below S2.
Attention to the diagnosis is often directed initially during evaluation of associated genitourinary or gastrointestinal malformations. Most common GU malformations include renal agenesis and hydronephrosis, whereas associated GI anomalies are typically anal atresia and imperforate anus. Other than lumbosacral agenesis, patients may also have associated vertebral segmentation anomalies and the entire spine should be screened for complete evaluation. There is an association with diabetic embryopathy, especially in diabetic pregnant women on insulin.
Ultrasound screening in the first trimester may demonstrate a shortened crown-rump length, whereas second trimester fetal survey can better demonstrate the sacral agenesis as well as associated genitourinary malformations.
References: Barkovich AJ. Congenital anomalies of the spine. In: Barkovich AJ, Raybaud C. (eds). Pediatric neuroimaging, 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2011.
Stroustrup Smith A, Grable I, Levine D. Case 66: caudal regression syndrome in the fetus of a diabetic mother. Radiology 2004;230(1):229-233.
4 Incidental finding on an MRI lumbar spine performed for low back pain in an otherwise healthy patient. Key images from an MRI are provided below.
|
4a Which of the following is the most likely diagnosis?
A. Fibrolipoma
B. Dermoid
C. Tethered cord
D. Lipomyelocele
4b Which of the following associations are seen with this entity?
A. Conus medullaris terminates at a normal position.
B. Associated with spinal dysraphism
C. Patients often have neurologic symptoms.
D. Vertebral segmentation anomalies
View Answer
4b Answer A. Conus medullaris terminates at normal position.
|
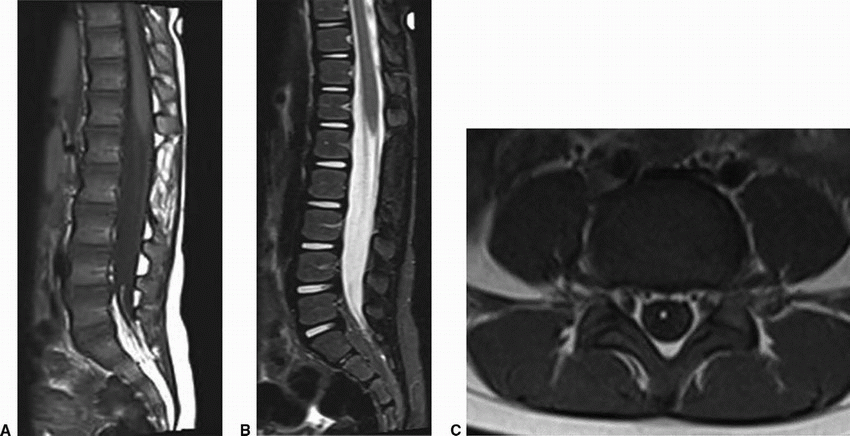
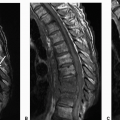
Imaging Findings: Sagittal T1w image demonstrates high signal within the filum at L4-S1 level, (arrow A) which is suppressed on the STIR images. Note normal position of the conus (arrow B). The distal fatty filum shows an abnormal dorsal location and appears tethered to the distal thecal sac. Axial T1 images with fat signal within the distal filum, which in this case, is not abnormally thickened. Findings compatible with a fatty filum or fibrolipoma.
Discussion: Fibrolipoma of filum terminale or fatty filum. Fatty filum refers to detection of fat in an otherwise normal size filum (transverse diameter <2 mm) in an asymptomatic patient. It is most commonly an incidental finding, which does not warrant further investigation.
Differential Diagnosis: It is important to differentiate from other fat-containing lesions such as intraspinal lipoma (larger in size), dermoid/epidermoid (more complex appearing) lipomyelocele (associated with posterior spinal fusion anomalies), and tethered cord (low-lying conus). MRI classically depicts high T1 signal within the filum, which is suppressed on fat-saturated sequences.
References: Barkovich AJ. Congenital anomalies of the spine. In: Barkovich AJ, Raybaud C. (eds). Pediatric neuroimaging, 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2011.
Bulsara KR, Zomorodi AR, Enterline DS, et al. The value of magnetic resonance imaging in the evaluation of fatty filum terminale. Neurosurgery 2004;54(2):375-379; discussion 379-380.
5 Chronic low back pain without radiculopathy or neurologic symptoms. An MRI was performed for further assessment. Key images are shown below.
 Images courtesy of Dr. Mai Lan Ho |
Based on the above images, what is the most likely diagnosis?
A. Syringomyelia
B. Terminal ventricle
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


