Fig. 1.1
Neurulation (dorsal induction). Simplified schematic drawing of the neurulation shows neural tube formation from the surface ectoderm induced by notochord. Proliferation of the neural ectoderm produces neural groove and fold and finally the tube and separated from surface ectoderm
1.6.2 Vesicle and Flexure Formation (Ventral Induction)
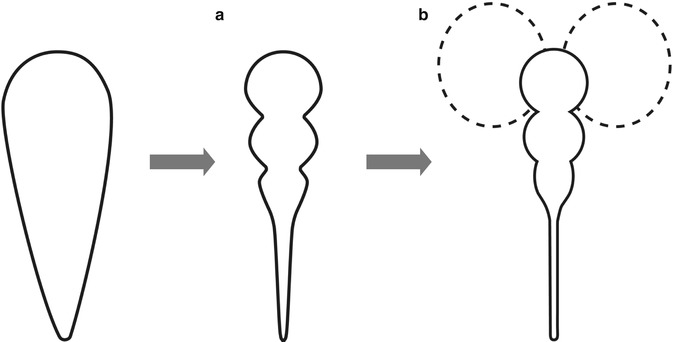
Fig. 1.2
Vesicle and flexure formation (ventral induction). Simplified schema shows expansion and constriction of neural tube forms prosencephalon, mesencephalon, and rhombencephalon (a). Telencephalons form from the prosencephalon (b)
1.6.2.1 Congenital Anomaly of the Brain
1.6.2.1.1 Encephaloceles
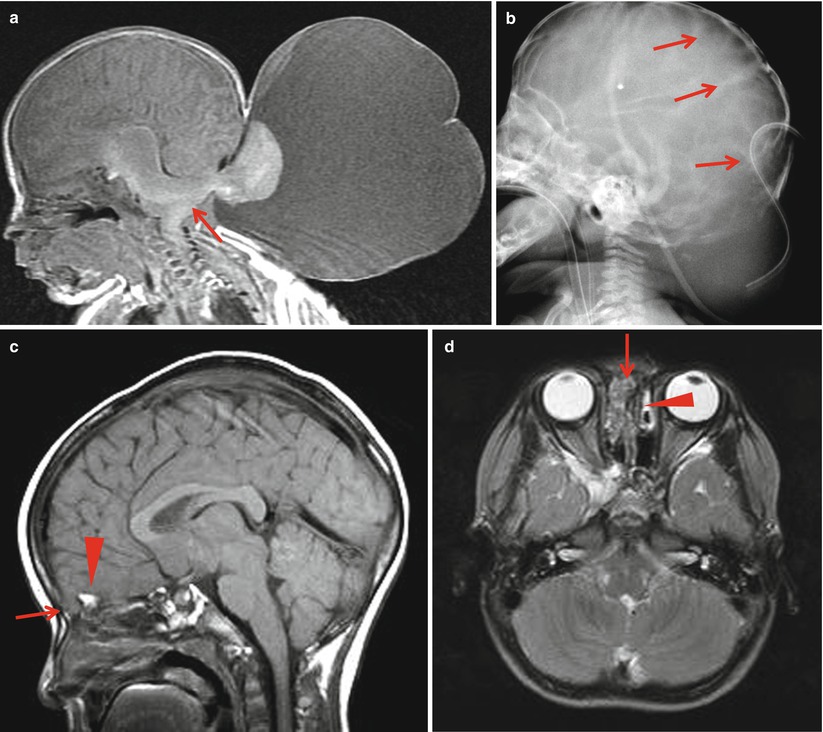
Fig. 1.3
Encephaloceles. (a) Large occipital encephalocele shows herniation of the cerebellum (arrow) and CSF through the occipital defect. Chiari malformation is accompanied. (b) Postoperative plain skull radiograph shows lacunar skull (arrows). (c, d) Frontoethmoidal encephalocele shows herniation of the brain parenchyma (arrows) through the foramen cecum anterior to the crista galli (arrowheads)
1.6.2.1.2 Chiari Malformation in Myelomeningocele
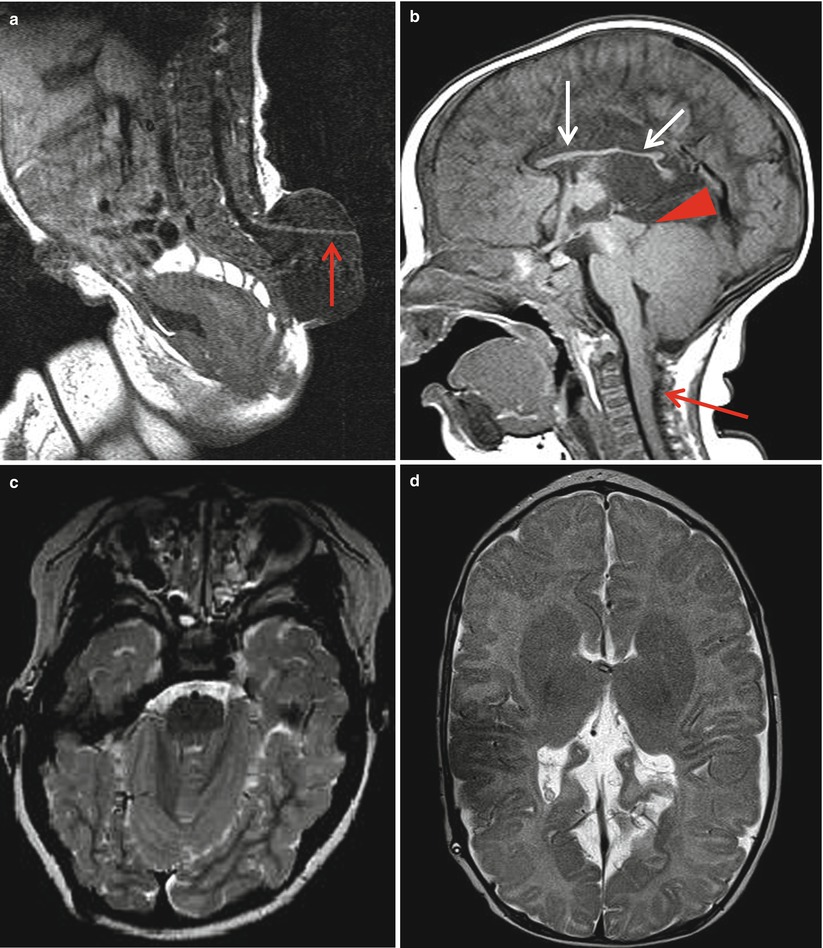
Fig. 1.4
Chiari malformation in myelomeningocele. (a) Herniated distal code (arrow) is continuous with the neural placode in the outer surface of the meningocele. Overlying skin defect is also present. (b) Sagittal image shows downward herniation of the medulla and cerebellar vermis. The fourth ventricle is narrow and elongated and extends down into the foramen magnum. The cervicomedullary kink is present at the C2 to C3 level. The tectum shows posterior beaking. Dysplastic corpus callosum shows scalloped thinning due to longstanding hydrocephalus (white arrows). (c) Axial T2-weighted image shows obliteration of the CSF space in the posterior fossa and squeezed appearance of the cerebellum. (d) Axial T2-weighted image shows dysplastic corpus callosum and falx
1.6.2.1.3 Holoprosencephaly, Semilobar Type
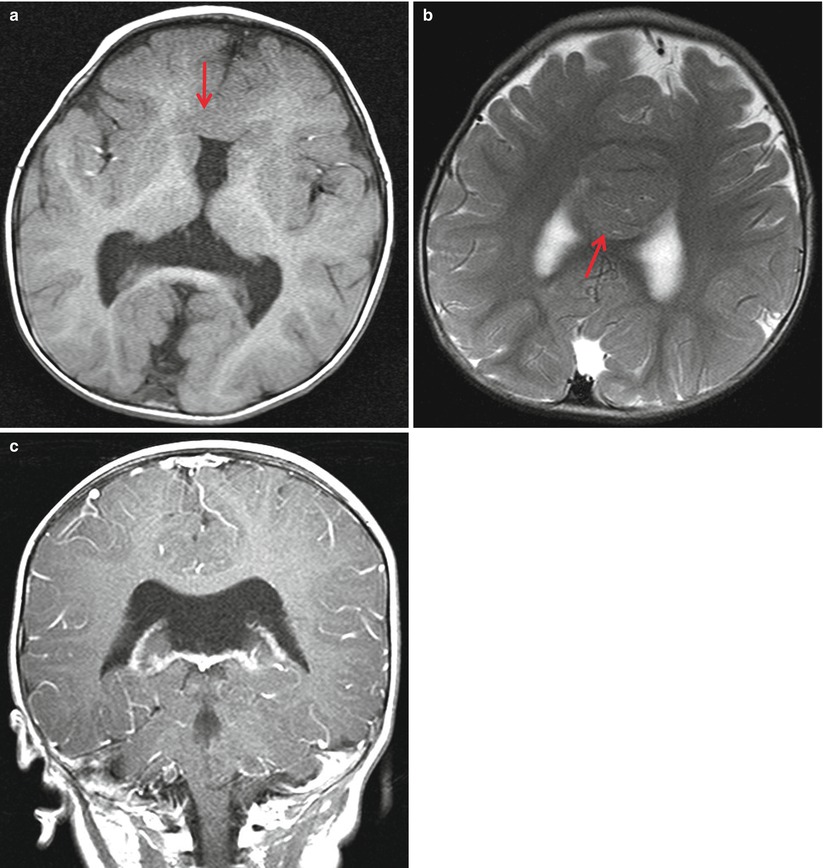
Fig. 1.5
Semilobar holoprosencephaly. (a) Frontal horn is hypoplastic and septum pellucid is absent. Occipital horn is well formed. Hemispheric connection (arrow) is seen anterior to the frontal horn instead of corpus callosum. (b) Interhemispheric gyral connection is evident over the lateral ventricles (arrow). (c) Coronal image shows fusion of the lateral ventricles in the posterior portion
1.6.2.1.4 Schizencephaly
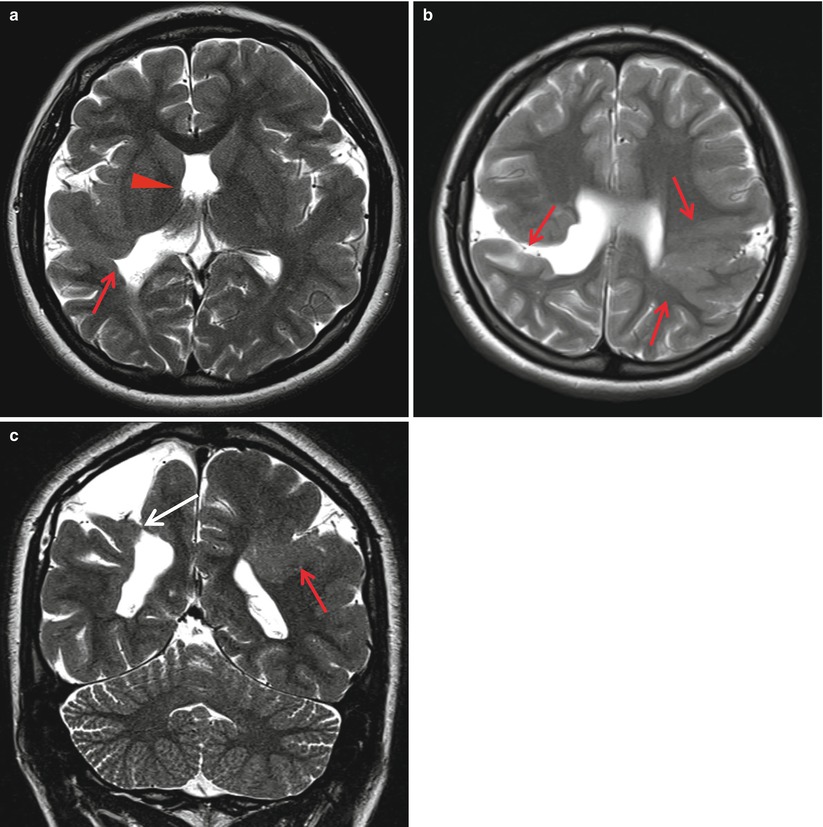
Fig. 1.6
Schizencephaly. (a) Thickened layer of gray matter extends from the cortex to the ventricular surface in the temporo-occipital region. Focal outpouching of the ventricle shows the opening of the cleft into the ventricle (arrow). Septum pellucidum is absent (arrowhead). (b, c) Open-lip schizencephaly (white arrow) shows CSF filling the cleft along the cortex and ventricle. Closed-lip schizencephaly (arrows) shows opposed cleft by the polymicrogyria
1.6.2.1.5 Lissencephaly
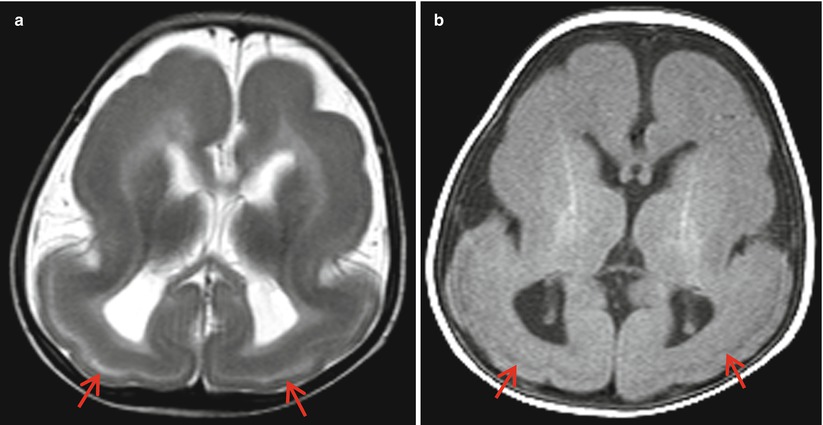
Fig. 1.7
Lissencephaly. (a) Axial T2-weighted image shows nearly smooth brain with shallow Sylvian fissure. The cortex is abnormally thick and outer linear band of high signal intensity (arrows) represents layer of laminar necrosis. (b) T1-weighted image shows low signal intensity of the laminar necrosis layer
1.6.2.1.6 Polymicrogyria
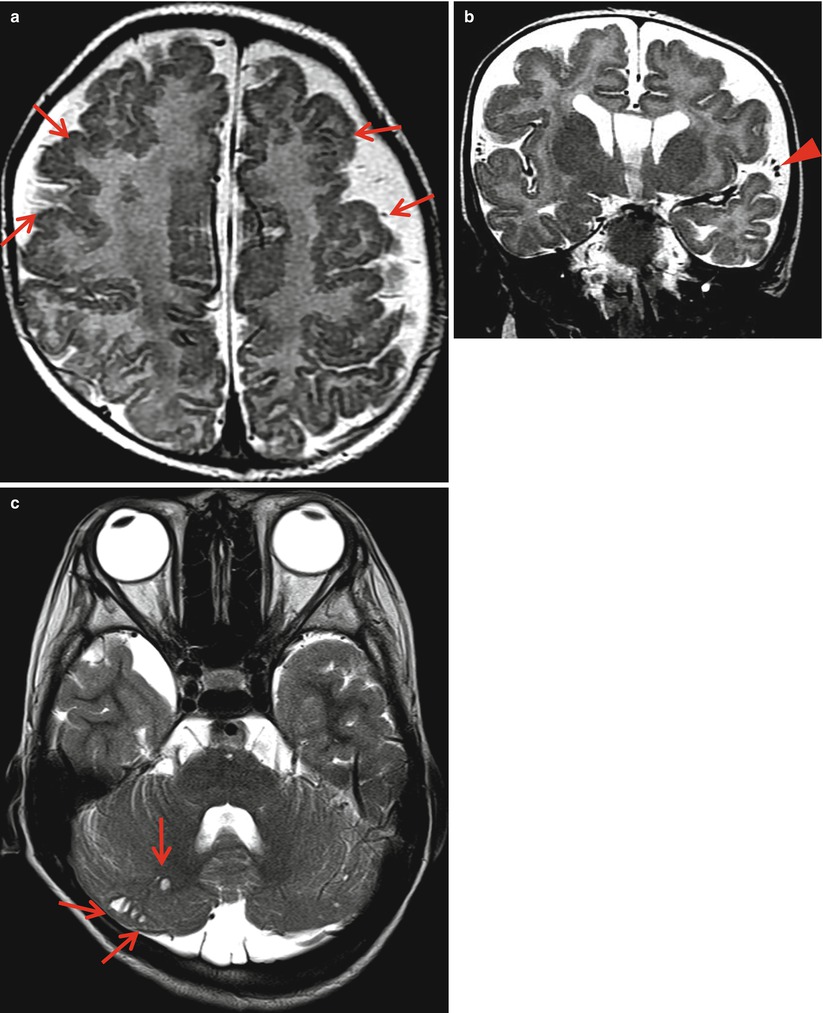
Fig. 1.8
Polymicrogyria. (a, b) T2-weighted image shows diffusely thickened irregular bumpy gyri (arrows) of both frontoparietal lobes with prominent overlying subarachnoid space. Sulcal abnormalities and prominent venous structures (arrowhead) are also present. (c) Cystic lesions along the surface of the cerebellum (arrows) suggest engulfed subarachnoid spaces due to cerebellar migration abnormalities
1.6.2.1.7 Heterotopia
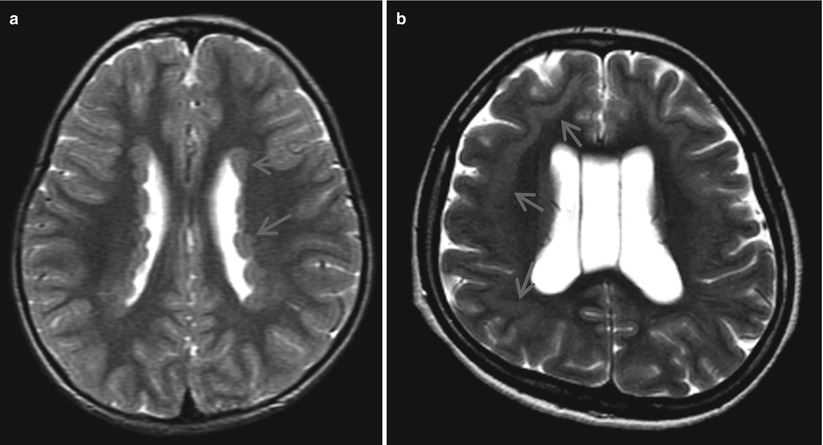
Fig. 1.9
Heterotopia. (a) Subependymal heterotopias show diffuse nodules of gray matter (arrows) along the both lateral ventricles. (b) Continuous layer of white matter (arrows) separates gray matter showing double cortex. The outer cortex shows smooth surface, suggesting pachygyria
1.6.2.1.8 Agenesis of the Corpus Callosum with Lipoma
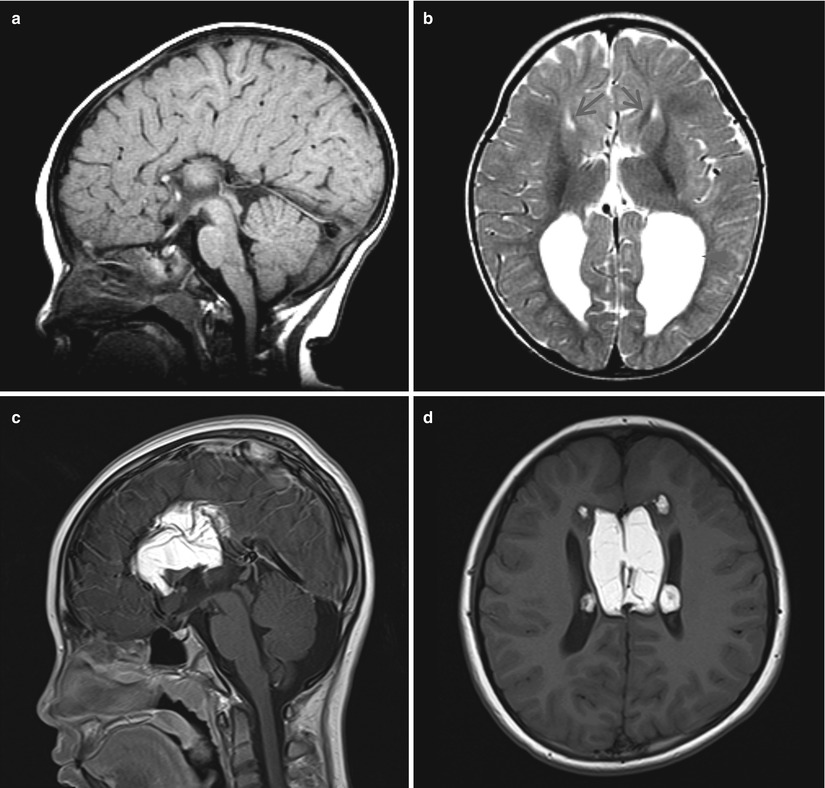
Fig. 1.10
Agenesis of the corpus callosum with lipoma. (a) Midsagittal image shows absent corpus callosum and the medial aspect of the cerebral sulci converge to the elevated third ventricle in radial arrangement. (b) Axial image shows parallel arrangement of the lateral ventricles and dilated occipital horns (arrowhead), so-called colpocephaly. Probst bundles are seen as curvilinear white matter (arrows) indenting the medial aspect of the lateral ventricles. (c, d) T1-weighted image shows lipomas in the interhemispheric region with sulcal and ventricular extension. Corpus callosum is absent
1.6.2.1.9 Dandy-Walker Malformation
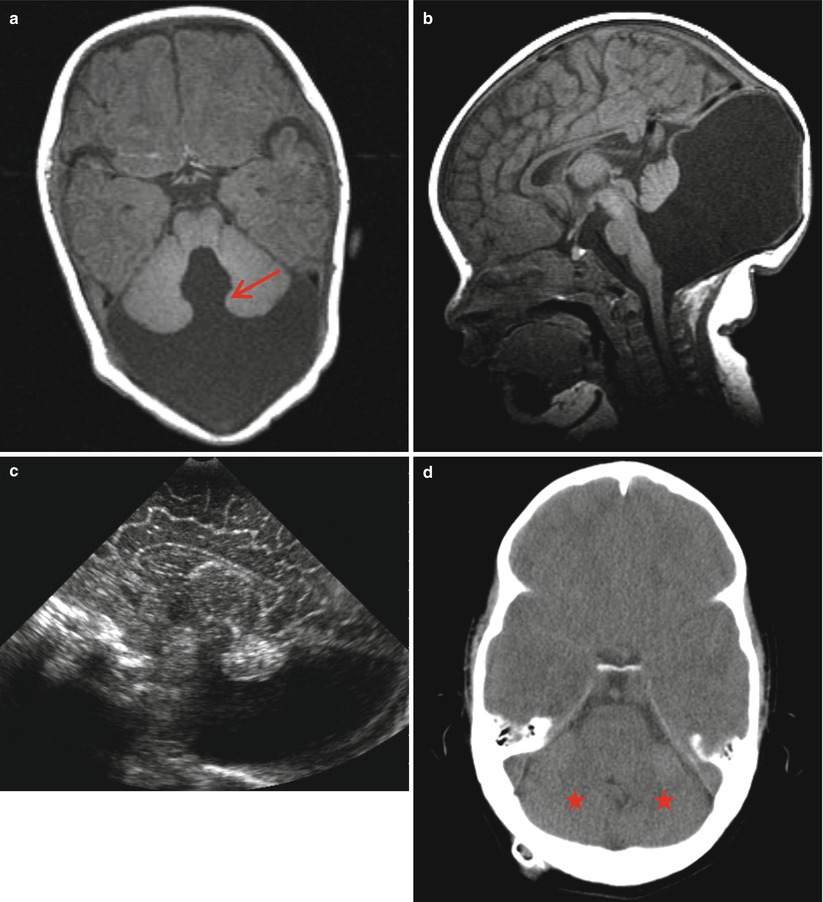
Fig. 1.11
Dandy-Walker malformation. (a) Axial image shows wide communication (arrow) of the fourth ventricle and the cyst displacing the hypoplastic cerebellum anteriorly. (b) Sagittal image shows large cyst occupying the inferior vermian region and elevating the tentorium and venous sinus upwardly. Cerebellar vermis is superiorly displaced. (c) Sagittal image of brain US reveals the large cyst-displacing vermis. (d) Follow-up CT after 2 years of cystoperitoneal shunt shows regrowth of the cerebellar hemispheres (arrows)
1.6.2.1.10 Joubert Syndrome
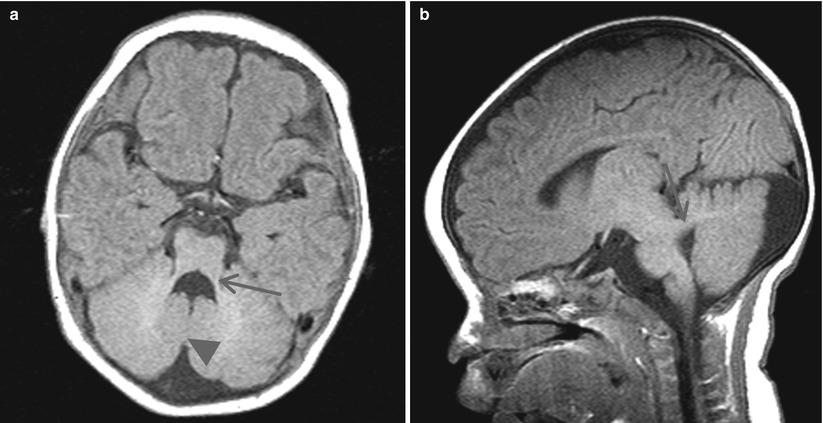
Fig. 1.12
Joubert syndrome. (a) Axial image shows batwing appearance of the fourth ventricle due to hypoplastic cerebellar peduncle (arrow) and cerebellar tonsillar opposition (arrowhead) instead of inferior vermis. (b) Sagittal image shows horizontal orientation of the superior cerebellar peduncle (arrow) with deformed fourth ventricle
1.6.2.2 Phakomatosis
1.6.2.2.1 Neurofibromatosis Type 1
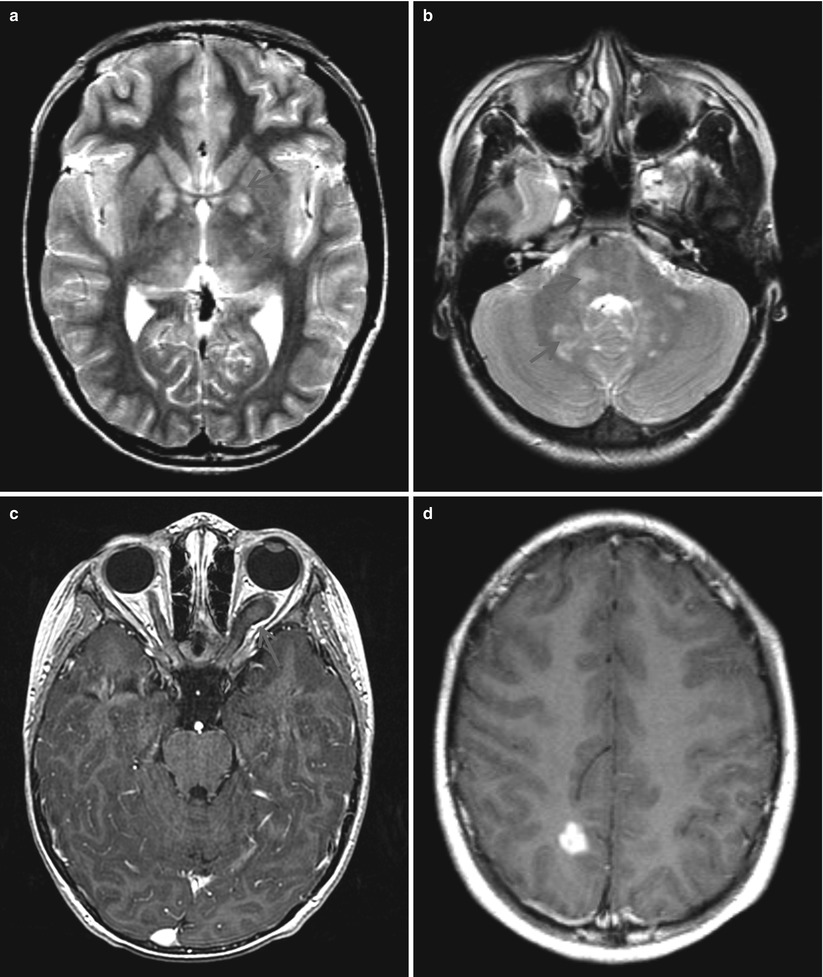
Fig. 1.13
Neurofibromatosis type 1. (a, b) Axial T2-weighted images show multiple nodular high signal intensity lesions (arrows) in the globus pallidus, posterior thalami, pons, and cerebellar white matter. (c) Postcontrast image shows diffuse thickening of the left optic nerve with mild enhancement and dural ectasia (arrow). (d) Pilocytic astrocytoma reveals as a discrete enhancing nodule in the right parietal region
1.6.2.2.2 Tuberous Sclerosis
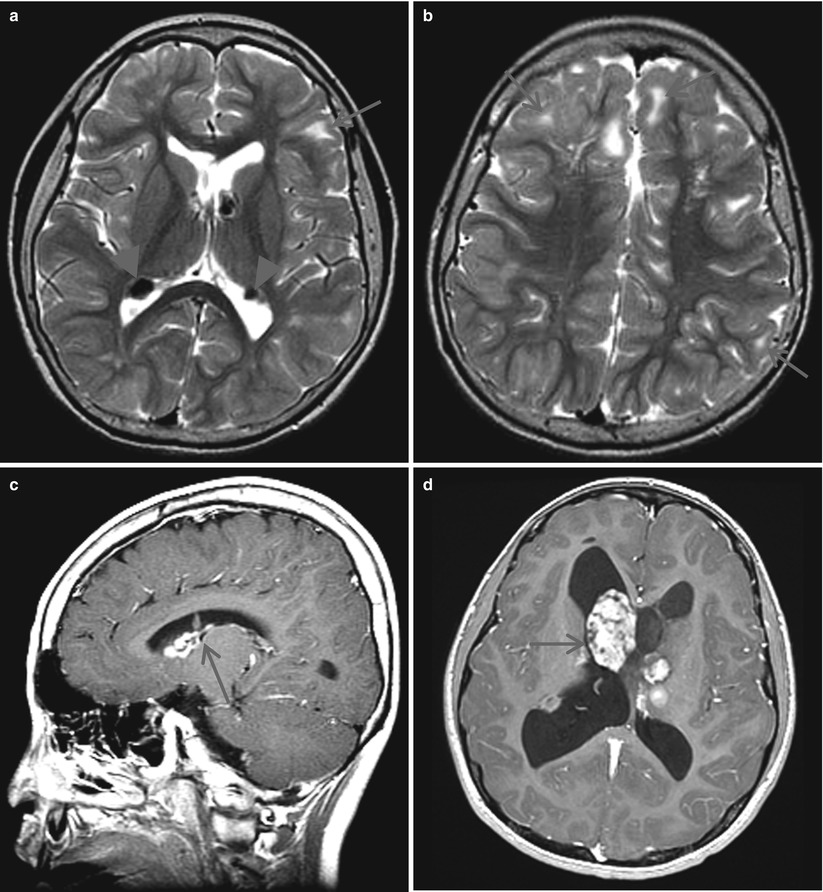
Fig. 1.14
Tuberous sclerosis. (a, b) T2-weighted image shows multiple subependymal tubers (arrowheads) along the wall of the lateral ventricles. The low signal intensities are due to calcifications. Cortical tubers (arrows) show multiple subcortical high signal intensity lesions with gyral expansion (arrow). (c) Postcontrast sagittal image shows strong homogenous enhancement of the subependymal tubers over the caudate nucleus. The tuber shows vertical orientation (arrow). (d) The large enhancing mass lesion obstructing the foramen of Monro, suggesting subependymal giant cell astrocytoma (arrow)
1.6.2.2.3 Sturge-Weber Syndrome
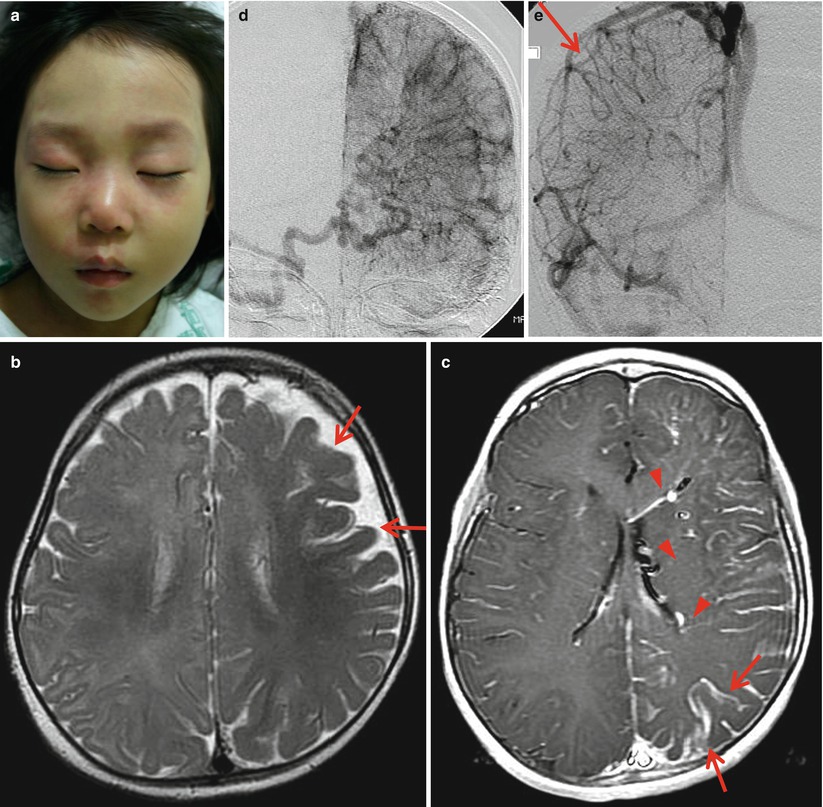
Fig. 1.15




Sturge-Weber syndrome. (a) Facial port-wine nevi located over the orbital and nasal region. (b) T2-weighted image shows atrophic gyri over the left hemisphere and exaggerated low signal intensities of the left hemispheric gyri (arrows). (c) Postcontrast image shows diffuse enhancement of the leptomeningeal angiomatosis in the left cerebral hemisphere (arrows) and prominent deep and ependymal veins (arrowheads). (d) Venous phase of the right vertebral angiography shows indistinct superficial cortical veins and prominent deep veins. (e) Normal superficial veins (arrow) are well demonstrated in the right cerebellum
Related posts:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
