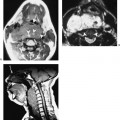
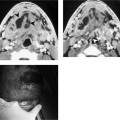
Chapter 209 Congenital anomalies of the second branchial apparatus arise from anomalous embryogenesis of a component of the second branchial complex. These are the most common branchiogenic anomalies and constitute 95% of all branchial abnormalities. Cysts are the most common malformation and usually present at between 10 and 40 years of age. Other malformations consist of sinuses and fistulas. There is no consistently reported gender predilection for these lesions. Branchial cleft cysts (BCC) are thought by most authors to result from incomplete obliteration of the epithelial-lined cervical sinus. BCC may occur anywhere along the developmental path of the second branchial complex from the tonsillar fossa to the level of the hyoid bone. The typical location is along the anterior border of the sternocleidomastoid muscle, lateral to the jugular vein at the level of the carotid bifurcation. BCC are classified by Bailey into four types (Fig. 209–1). Type 1 are superficial lesions located along the anterior border of the sternocleidomastoid muscle just beneath the superficial cervical fascia. Type 2 BC are the most common form and represent deeper lesions that abut the carotid sheath. Type 3 lesions are cysts that pass medially between the internal and external carotid arteries and extend inward toward the lateral wall of the pharynx. Occasionally, type 3 cysts have been noted to extend cranially as far as the skull base. Type 4 is a BCC that is lined by columnar epithelium. A sinus arising from the second branchial apparatus is felt to occur from a communication connecting an incompletely obliterated cervical sinus and the skin. Second branchial groove fistulas are thought to develop if the second branchial groove communicates with the second branchial pouch. The result is a fistula with an internal opening within the tonsillar fossa, often adjacent to the posterior tonsillar pillar, and an external opening along the anterior border of the sternocleidomastoid muscle. The fistulous tract is situated lateral to the ninth and twelfth cranial nerves. The tract may pass between the internal and external carotid arteries and pierce the platysma muscle just prior to its external communication.
Congenital Anomalies of the Second Branchial Apparatus
Epidemiology
Embryology
Cysts
Sinus
Fistula
Clinical Findings
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


