CHAPTER 33 Congenital Coronary Anomalies
DEFINITION
Anomalous coronary arteries can be grouped into three general categories. Angelini and colleagues1 have written one of the most complete works on this subject, and this text can serve as an excellent reference for additional study. Anomalies generally can be divided into three general classifications: (1) anomalies of origin and course (ectopic ostium within proper sinus, ostium outside normal sinus, and absent vessel); (2) anomalies of intrinsic coronary arterial anatomy (congenital stenosis of ostium, congenital aneurysms, and myocardial bridging); and (3) anomalies of coronary termination (fistulas) (Table 33-1).
TABLE 33-1 Classification of Coronary Anomalies
| Anomalies of origin and course |
Anomalous coronary artery from the opposite sinus of Valsalva |
| Anomalies of Intrinsic Coronary Arterial Anatomy |
| Anomalies of Termination |
| Coronary artery fistula |
PREVALENCE AND EPIDEMIOLOGY
Congenital anomalies of the coronary arteries affect about 1.3% (range 0.2% to 5.6%) of individuals.2–10 Approximately 80% of anomalies are considered benign without significant clinical sequelae; the remaining 20% can potentially cause symptoms, and may be responsible for significant disease.3
MANIFESTATIONS OF DISEASE
Clinical Presentation
Presentation depends greatly on the specific anomaly. Most coronary artery anomalies are benign and never have any clinical symptoms. These are usually detected as incidental findings. Other anomalies are potentially significant and are sometimes ominously termed malignant or potentially lethal; these increase the risk of myocardial ischemia and sudden death because their position or orientation may lead to coronary flow compromise.11–15 Although anomalies are uncommon, they can have a substantial impact on premature cardiac morbidity and mortality among young adults. Eckart and associates16 found coronary anomalies present in more than 30% of sudden nontraumatic deaths in young individuals.
Imaging Indications and Algorithm
Noninvasive imaging has emerged as the preferred way to diagnose and evaluate coronary anomalies. Echocardiography can often detect anomalous origins and even some anomalous courses or, as in the case of larger fistulas, anomalous terminations. Electron-beam CT and MR angiography are useful for the comprehensive diagnosis of anomalous coronary arteries.17–22 More recently, multidetector CT has proved to be useful in the detection and characterization of anomalous coronary arteries.23–28
IMAGING TECHNIQUE AND FINDINGS
Computed Tomography
Cardiac multidetector CT using contrast-enhanced technique is capable of detecting and characterizing coronary artery anomalies. Most anomalies are incidental findings and are frequently detected when the coronary arteries are being evaluated for atherosclerotic stenoses. The same CT angiographic technique is used when imaging coronary anomalies and atherosclerotic coronary artery disease. This technique is discussed in depth in Chapter 9.
DIFFERENTIAL DIAGNOSIS
Anomalies of Origin and Course
Anomalous Origin of a Coronary Artery from the Opposite Sinus of Valsalva
There are several potential courses for an anomalous LCA arising from the right sinus of Valsalva or the RCA (Fig. 33-1). Diagnosis of the exact course is important because it determines if intervention is necessary. There are four possible pathways for the anomalous LCA: (1) between the aortic root and the pulmonary artery (interarterial course), (2) a transseptal (intraseptal or subpulmonic) course, (3) anterior to the right ventricular outflow tract (anterior or prepulmonic course), and (4) posterior to the aortic root (retroaortic course). Although the anterior, posterior, and septal (subpulmonic) courses are benign, an interarterial course carries a high risk for sudden cardiac death.29,30
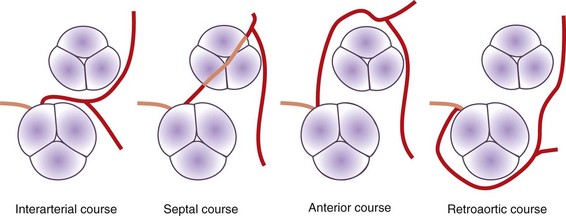
 FIGURE 33-1
FIGURE 33-1Axial reconstructions from a multidetector CT coronary angiogram can depict the anatomic course. The exact position and course of the anomalous artery can be viewed in relation to the aortic root and pulmonary artery (Fig. 33-2). The LCA arises from the right sinus of Valsalva or directly from the RCA in 0.10% of patients, and an interarterial course is present in approximately 75% of these patients.31

 FIGURE 33-2
FIGURE 33-2Three-dimensional volume rendered multidetector CT images of the coronary arteries and aortic root can also be helpful in depicting the course and anatomic relationships. An anomalous coronary artery originating from the opposite sinus of Valsalva can cause syncope, myocardial infarction, and sudden death in the absence of critical, fixed stenosis. Patients with an anomalous LCA that takes an interarterial course have a high risk for sudden cardiac death because of the acute angle of the ostium, the stretch of the intramural segment of the anomalous artery, or the compression between the commissures of the right and left coronary cusps.1,31 This anomalous LCA may narrow the origin or proximal aspect of the vessel and limit flow. An anomalous interarterial coronary artery is frequently an underlying cause for sudden death in young athletes. Often, MRI can also show an anomalous coronary artery with an interarterial course (Fig. 33-3).
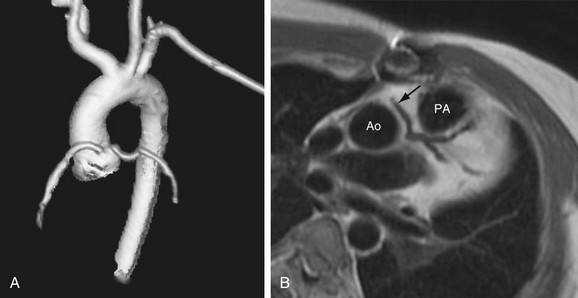
 FIGURE 33-3
FIGURE 33-3


