Abstract
Cysts of the umbilical cord have been reported in all trimesters. The clinical significance and prognosis of cord cysts vary depending on the gestational age at diagnosis, persistence of the cyst, and associated structural or chromosomal abnormalities. Most cysts that are diagnosed in early pregnancy disappear by 14 weeks’ gestation and are not associated with an adverse pregnancy outcome. Umbilical cord cysts that persist into the second and third trimester of pregnancy, however, are associated with fetal aneuploidy or fetal structural defects. On ultrasound (US), cord cysts have the appearance of anechoic structures located within the fetal umbilical cord. They can occur as a solitary lesion or as multiple lesions, and they do not demonstrate evidence of flow during color Doppler US. The differential diagnosis of this finding includes true cysts, pseudocysts, allantoic cysts, and hematomas. Both true cysts and pseudocysts that persist in the second and third trimesters are associated with congenital anomalies and aneuploidy. Thus the US finding of a cord cyst should prompt a thorough search for other malformations. A cord cyst detected in the first trimester should be reassessed with US examination in the second trimester. Although there are currently no prenatal or postnatal treatment options for fetuses with umbilical cord cysts, the prognosis for fetuses with this finding, in the absence of additional US or chromosomal abnormalities, is excellent.
Keywords
umbilical cord cyst, anechoic, pseudocyst
Introduction
The widespread use of high-resolution ultrasound (US) in routine obstetric care has led to greater detection of placental and umbilical cord abnormalities. Cysts of the umbilical cord have been reported in all trimesters. The clinical significance and prognosis of cord cysts vary depending on the gestational age at diagnosis, persistence of the cyst, and associated structural or chromosomal abnormalities.
Disorder
Definition
A cord cyst is defined as an echolucent area within the umbilical cord.
Prevalence and Epidemiology
First-trimester umbilical cord cysts have been reported to occur in approximately 0.4% to 3.4% of pregnancies. Most cysts (approximately 80%) that are diagnosed in early pregnancy resolve by 12 to 14 weeks’ gestation and are not associated with an adverse pregnancy outcome. Umbilical cord cysts that persist into the second and third trimester of pregnancy, however, are associated with an increased risk of fetal aneuploidy or fetal structural defects.
Etiology, Pathophysiology, and Embryology
Most cord cysts detected in the first trimester are transient and disappear by 14 weeks’ gestation. These transient cysts are not associated with an additional risk to the pregnancy. Umbilical cord cysts are classified as either true cysts or pseudocysts. True cysts develop from remnants of the allantois or omphalomesonephric duct. Histologically, they are lined by either columnar, mucin-secreting cells (omphalomesonephric), cuboidal cells resembling transitional epithelium (allantoic), or amniotic epithelium (amniotic). Umbilical cord cysts are located more frequently at the fetal abdominal cord insertion site and range in size from 4–60 mm. Pseudocysts are encountered more frequently than true cysts and are generally located near the fetal end of the umbilical cord as well. They contain no epithelial lining and represent mucinous degeneration or localized edema of Wharton jelly. Differentiation between a true cyst and a pseudocyst on US is challenging because both manifest as anechoic structures primarily located toward the fetal cord insertion site.
Regardless of the histologic diagnosis, both true cysts and pseudocysts that persist in the second and third trimesters are associated with congenital anomalies and aneuploidy.
The association between adverse fetal outcomes and umbilical cord cysts seen in the second and third trimester has been demonstrated in several studies. However, the overall prevalence of associated abnormalities is unclear, with reports ranging from 20% to 100%. Associated anomalies include patent urachus, multiple vascular anomalies, congenital heart disease, and umbilical hernia, as well as intrauterine growth restriction and aneuploidy. An “hourglass” appearance from the bladder to an umbilical cord cyst can indicate significant disease ranging from patent urachus to bladder exstrophy, and the need for birth at a tertiary center with pediatric urologic consultation readily available.
Manifestations of Disease
Clinical Presentation
Cord cysts are diagnosed during US examination at any time in pregnancy.
Imaging Technique and Findings
Ultrasound.
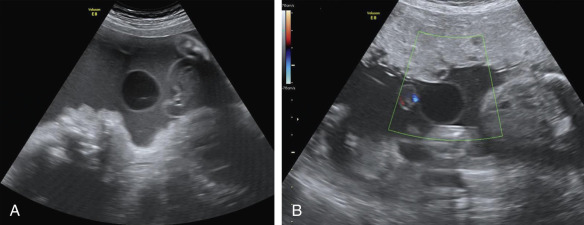
Cord cysts are anechoic structures located within the fetal umbilical cord. They can occur as a solitary lesion or as multiple lesions and range in size from 4–60 mm. Although these cysts are usually located near the fetal end of the umbilical cord, they can be located anywhere along the length of the cord. Cord cysts can be axial, within the center of the umbilical cord and displacing the umbilical vessels, or paraxial, on the periphery of the cord. Use of color Doppler demonstrates no flow ( Fig. 102.1 ).