CHAPTER 36 Coronary Artery Aneurysms
DEFINITION
Coronary artery aneurysm (CAA) is defined as a dilation more than 1.5 times the diameter of adjacent normal segments.1 It was first described by Morgagni in 17812,3; the first case report was published by Bougon in 1812,1,4 and the first documented case with angiography was published by Munker in 1958.5,6 Before the advent of coronary angiography, CAAs were detected primarily at postmortem examination; however, most cases today are incidental findings on angiography.
PREVALENCE AND EPIDEMIOLOGY
The reported incidence of CAAs ranges from 0.2% to 4.9% among patients undergoing evaluation for coronary disease.1,5 They occur predominantly in men at a ratio of almost 3 : 1.4 CAAs are predominantly caused by atherosclerosis (52%). They may be single or multiple, may be focal or diffuse, and can involve various segments of the coronary circulation. They most commonly involve the right coronary artery (Fig. 36-1) followed by the left anterior descending (Fig. 36-2) and the left circumflex (Fig. 36-3) arteries.4
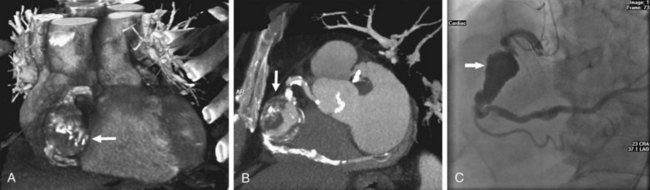
 FIGURE 36-1
FIGURE 36-1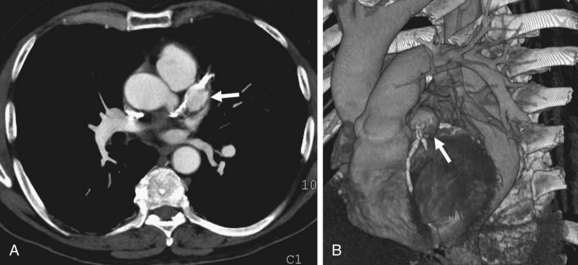
 FIGURE 36-2
FIGURE 36-2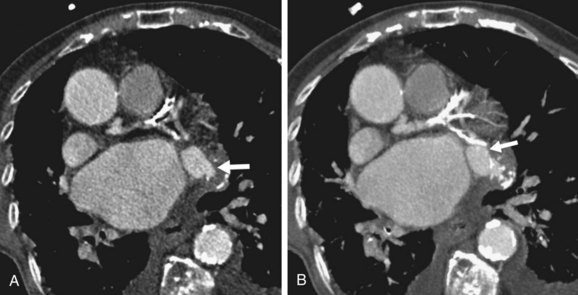
 FIGURE 36-3
FIGURE 36-3Atherosclerotic aneurysms of the left main coronary artery are rare, but have been reported.7 Other important etiologies include congenital (17%), mycotic-embolic (11%), dissecting (11%), syphilitic (4%), and unclassified (5%).4 Although most cases worldwide are secondary to atherosclerosis, systemic inflammatory diseases such as Takayasu arteritis (Fig. 36-4) and the mucocutaneous lymph node syndromes of Kawasaki disease (Fig. 36-5) account for many cases in East Asia.8 Modern interventional techniques have also resulted in iatrogenic causes of CAAs. In the current era of percutaneous intervention, CAAs can be seen secondary to balloon angioplasty or stent deployment.9 The increasing use of coronary artery bypass grafting techniques has resulted in numerous reports of saphenous vein graft aneurysms (Fig. 36-6), although they remain uncommon.
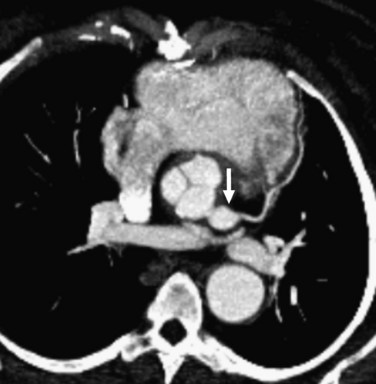
 FIGURE 36-4
FIGURE 36-4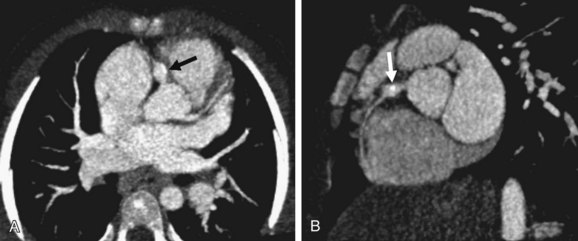
 FIGURE 36-5
FIGURE 36-5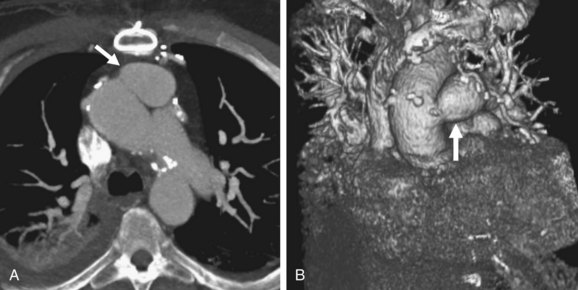
 FIGURE 36-6
FIGURE 36-6Although CAAs may be found at any age, atherosclerotic subtypes are predominant later in life, whereas congenital (Figs. 36-7 and 36-8), mycotic-embolic, and dissecting types are found in younger age groups. Multiple CAAs in childhood and adolescence are usually late complications of Kawasaki disease (Fig. 36-9).10
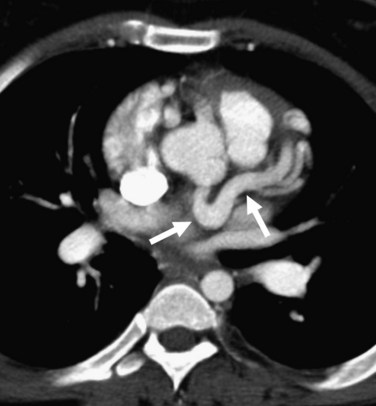
 FIGURE 36-7
FIGURE 36-7Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


