Craniocervical Dissociation
James C. Darsie
CLINICAL HISTORY
18-year-old male pedestrian struck by a car traveling 55 mph and thrown 100 feet. The patient suffered a pulseless electrical activity arrest in the field and now presents with fixed and dilated pupils and no neurologic responses.
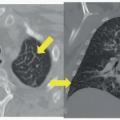
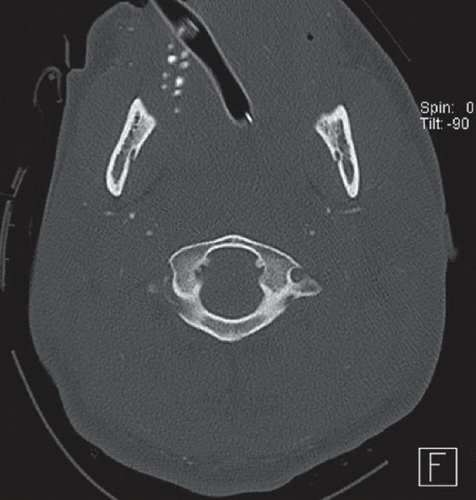 FIGURE 89A |
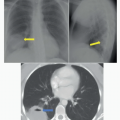
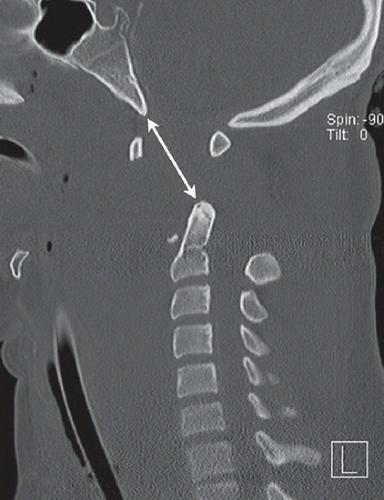 FIGURE 89B |
 FIGURE 89C |
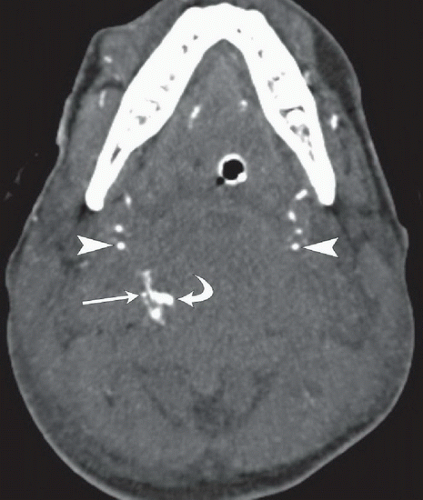 FIGURE 89D |
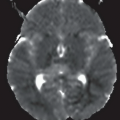
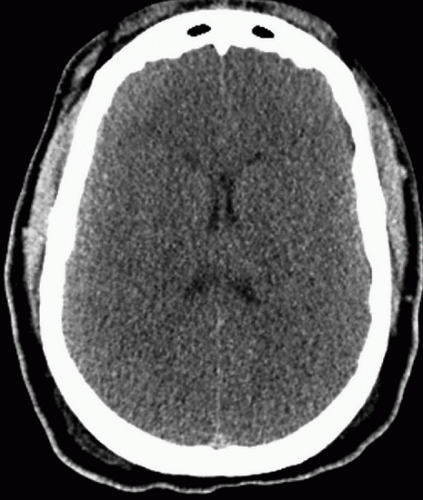 FIGURE 89E |
FINDINGS
Figure 89A: Axial bone window CT image at the level of C1 demonstrates an intact C1 ring; however, the dens is not visualized in its normal position behind the anterior C1 arch. Figures 89B and 89C: Sagittal bone window CT images through the cervical spine demonstrate complete craniocervical dissociation, evidenced by marked widening of the dens-basion interval (double arrow), along with widening of the C1-C2 interspinous distance on the midsagittal image (Fig. 89B). A small avulsed bone fragment arising from the inferior aspect of the anterior C1 arch remains in normal position anterior to the dens; however, the remainder of C1 is superiorly distracted. On the parasagittal image (Fig. 89C) there is a large gap between the lateral masses of C1 and C2, while the atlantooccipital joint remains located. Figure 89D: Axial image from a CTA of the neck demonstrates extravasated contrast (curved arrow) adjacent to a small, opacified right vertebral artery (thin arrow). The left vertebral artery is not seen. Note also, the markedly diminished caliber of the internal carotid arteries (arrowheads). Figure 89E: Axial unenhanced head CT image demonstrates diffuse brain edema with complete loss of gray-white matter differentiation.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


