Abnormalities of Diaphragmatic Motion: Diaphragmatic Paralysis, Weakness, and Eventration
Etiology, Prevalence, and Epidemiology
The diaphragm is the primary muscle of ventilation, and dysfunction of the diaphragm is an underrecognized cause of dyspnea. Dysfunction of the diaphragm can be classified as paralysis, weakness, or eventration and is usually suggested by elevation of a hemidiaphragm on chest radiography. Some of the more common causes of unilateral diaphragmatic paralysis are compression or invasion of the phrenic nerve by a neoplasm or iatrogenic injury during birth or open heart surgery. Other common causes include trauma (natural or surgical) and cardioplegia for cardiac surgery (“phrenic frostbite”). Less common causes are herpes zoster, West Nile virus, cervical spondylosis, poliomyelitis, amyotrophic lateral sclerosis, and pneumonia. However, in many cases the etiology is unknown.
The most common cause of bilateral diaphragmatic paralysis is spinal cord injury. Bilateral diaphragmatic paralysis or weakness can also be caused by generalized neuromuscular syndromes, such as amyotrophic lateral sclerosis or myasthenia gravis. Bilateral paralysis occurs occasionally after cardioplegia for cardiac surgery; this form is usually reversible with time.
Eventration is a congenital anomaly consisting of failure of muscle development of part or all of one or both hemidiaphragms. On pathologic examination a totally eventrated hemidiaphragm consists of a thin membranous sheet attached peripherally to normal muscle at points of origin from the rib cage. Complete eventration almost exclusively affects the left hemidiaphragm. Partial eventration is much more common than the complete form. It affects men and women with equal frequency. It usually involves the anteromedial portion of the right hemidiaphragm and only rarely the left, but it can involve the central portion of either cupola.
Clinical Presentation
Unilateral diaphragmatic paralysis or weakness is usually asymptomatic and is found incidentally on chest radiographs obtained for a different reason. Dyspnea with mild to moderate effort may develop in patients with underlying lung disease. Patients with bilateral diaphragmatic paralysis or weakness usually have severe respiratory symptoms, mainly dyspnea and orthopnea, sometimes with a sense of suffocation when supine or when immersed in water. Most patients eventually develop respiratory failure. Bilateral hemidiaphragmatic weakness can also occur after prolonged mechanical ventilation and may signal that the patient cannot be weaned from the ventilator.
Eventration is usually asymptomatic but may become symptomatic if the eventration is large or the patient is obese because obesity can raise intraabdominal pressure and further compromise diaphragmatic function.
Manifestations of Diaphragm Dysfunction
Radiography and Fluoroscopy
The paralyzed or weak hemidiaphragm is elevated and has an accentuated domed shape on the posteroanterior radiograph. Elevation of the posterior aspect of the hemidiaphragm, best shown on the lateral radiograph ( Fig. 78.1 ), is a helpful radiographic feature of a paralyzed or weak hemidiaphragm but is usually absent in a large eventration. The lung adjacent to a paralyzed hemidiaphragm often has subsegmental atelectasis resulting from elevation and reduced motion. If the paralysis is on the left, the stomach and splenic flexure of the colon relate to the inferior surface of the hemidiaphragm and usually contain more gas than normal.

Complete eventration of a hemidiaphragm is a rare, congenital abnormality that is almost always on the left. On the other hand, partial eventration is common; it may be acquired, and it usually affects patients older than 60 years, typically involving the anteromedial portion of the right hemidiaphragm. For the rest of this chapter we will use eventration to mean partial eventration .
A small eventration usually has two distinct arcs on the lateral projection, with the higher arc representing the thinned portion ( Fig. 78.2 ). A large eventration may be mistaken for a paralyzed or weak hemidiaphragm, but the pattern of elevation is different; in eventration the hemidiaphragm has a steeper arc and descends posteriorly to normal height, whereas a paralyzed or weak hemidiaphragm has a shallower arc and stays elevated posteriorly all the way to the chest wall. Subsegmental atelectasis near the elevated hemidiaphragm is often not as great as with paralysis because the hemidiaphragm usually maintains some degree of motion.

Eventration involving the anterior right hemidiaphragm can be distinguished from a Morgagni hernia by its contour on the lateral radiograph. With eventration, the entire contour of the hemidiaphragm is visible on lateral view, whereas with Morgagni hernia the contour is obscured by the hernia contents and surrounding mediastinal tissue.
The usual imaging test to demonstrate hemidiaphragmatic paralysis, weakness, or eventration is fluoroscopy, but ultrasonography or dynamic magnetic resonance (MRI) can be used.
Although diaphragm fluoroscopy is often called the sniff test, sniffing is not the most important part, and sniffing by itself does not diagnose paralysis. The diagnosis of paralysis requires observing quiet and deep inspiration. Absence of downward motion on slow, deep inspiration is the critical finding that indicates paralysis. Sniffing is best viewed as a stress test that elicits relative weakness (not only paralysis) of a hemidiaphragm. In pitting one hemidiaphragm against the other, sniffing is analogous to arm wrestling, in which the arm of the stronger opponent pushes forward, forcing the weaker opponent’s arm backward (i.e., paradoxically), even though the weaker arm is not paralyzed.
A thorough fluoroscopic examination includes watching the hemidiaphragms in both frontal and lateral projections with the patient upright and often also supine, particularly if the patient complains of dyspnea when lying down or is suspected to have bilateral paralysis. The lateral view is needed to show the excursion of the posterior portion of the diaphragm, which is usually more vigorous than the anterior portion. The lateral view also shows the anterior and upward movement of the chest wall on inspiration. The supine view is needed to reveal bilateral hemidiaphragmatic paralysis when the apparently normal diaphragm excursion on upright views is actually passive movement from use of the abdominal muscles. The supine view can also reveal weakness because the supine position provides a stress test of the diaphragm by making it work against the weight of the abdomen. Even decubitus positioning can be used if clinically relevant.
Performing the Fluoroscopic Sniff Test a
a Modified from reference .
This technique includes upright frontal and lateral views followed by semisupine and fully supine frontal views.
- 1.
Practice breathing maneuvers before fluoroscopy. Coach the patient in taking in a slow deep breath with the mouth open and then letting it out without forcing it or pursing the lips. Then coach the patient in sniffing. After exhalation of a slow deep breath, the patient should close the mouth and breathe in through the nose as hard, fast, and deeply as possible. Note that this maneuver should be a single long sniff, not a series of short sniffs.
- 2.
With the patient upright, adjust collimation to show the entire chest. Observe a couple of quiet breaths.
- 3.
Then observe a slow, deep breath. (“Take in a deep breath…now let it out.”)
- 4.
Observe a second deep breath and at the end of the expiration, tell the patient to close the mouth and sniff. “Take in a deep breath…now let it out….now close your mouth and sniff!”).
- 5.
Repeat steps 3 and 4.
- 6.
Turn the patient into the lateral position, with arms out of the field of view. Observe two quiet breaths, and then observe two deep breaths with the second one followed by the sniff. Repeat.
- 7.
Turn the patient back into the frontal position. Observe two deep breaths. Then observe two quiet breaths and note the resting positions of both hemidiaphragms at end expiration.
- 8.
Tilt the fluoroscopic table to 45 degrees elevation. Observe two deep breaths, then two quiet breaths, and again note the resting positions of both hemidiaphragms at end expiration.
- 9.
Tilt the fluoroscopic table to the supine position. Again observe two deep breaths, then two quiet breaths, and note the resting positions of both hemidiaphragms at end expiration.
- 10.
The examination can be recorded on video loops sent to a picture archiving and communication system or with movies burned to a digital video disc.
Interpreting the Fluoroscopic Sniff Test a
a Modified from reference .
- 1.
Normal findings
- A.
On quiet and deep inspiration both hemidiaphragms move downward as the anterior chest wall moves upward. Excursion is usually one rib interspace or more. On lateral view excursion is usually greater posteriorly, particularly on the right; it may be slightly asymmetric, and the right side may lag, particularly anteriorly.
- B.
On sniffing both hemidiaphragms move downward as the chest wall moves upward. (Chest wall motion may be attenuated compared to that on slow deep inspiration.) Excursion is again greater posteriorly. Some asymmetry is common, and the right hemidiaphragm may lag, particularly anteriorly. There may even be transient upward (paradoxical) motion, particularly of the right anterior hemidiaphragm.
- C.
When the patient is lowered to 45 degrees elevation and then to the supine position, excursion of both hemidiaphragms is usually less than with the patient upright. Also, there is often 1 to 2 cm upward displacement of the resting position of the hemidiaphragms.
- A.
- 2.
Paralysis of one hemidiaphragm
- A.
On deep breathing downward excursion is nearly or completely absent. There may be upward (paradoxical) motion on deep or even quiet breathing, and the mediastinum usually shifts away from the side of paralysis during inspiration.
- B.
On sniffing there is usually upward (paradoxical) motion.
- C.
On supine position there may be excess elevation of the resting position of the hemidiaphragm.
- A.
- 3.
Paralysis of both hemidiaphragms
- A.
Both hemidiaphragms are elevated, often with atelectasis in the lung bases.
- B.
Motion of the anterior chest wall in some cases may cause both hemidiaphragms to move upward on inspiration—that is, in the same (upward) direction as the chest wall rather than in the opposite (downward and orthograde) direction. It is important to recognize that the diaphragm is moving paradoxically when it moves in the same direction as the chest wall.
- C.
On upright views the excursion of both hemidiaphragms may appear to be normal if the patient is using abdominal muscles to passively move the diaphragm. (Tightening abdominal muscles on expiration pushes the diaphragm up, and relaxing them on inspiration allows the diaphragm to fall.) On supine and semisupine views this mechanism is defeated, and excursion of the hemidiaphragms is severely reduced.
- D.
On supine views there is excess elevation of the resting positions of both hemidiaphragms.
- A.
- 4.
Weakness of one or both hemidiaphragms
- A.
On deep inspiration downward excursion is less than one rib interspace. There may be upward (paradoxical) motion on deep or even quiet breathing. Hemidiaphragmatic weakness often becomes more obvious on rapid, deep inspiration, with the weak hemidiaphragm lagging behind the normal side.
- B.
On sniffing there may be upward (paradoxical) motion.
- C.
On supine views there may excess elevation of the resting position of the hemidiaphragm.
- A.
- 5.
Eventration of a hemidiaphragm
- A.
On deep breathing excursion of the eventrated segment is less than the rest of the hemidiaphragm. There may be transient upward motion of the segment on deep or even quiet breathing.
- B.
On sniffing there may be upward (paradoxical) motion of the segment. A rocking motion may ensue on lateral view, with the anterior eventrated segment moving upward while the posterior portion moves downward.
- C.
On supine position there may be excess elevation of the resting position of the eventrated segment.
- A.
Again, because upward (paradoxical) motion on sniffing could reflect weakness, eventration, or paralysis, the fluoroscopic diagnosis of hemidiaphragmatic paralysis is not based on sniffing but instead on the absence of downward motion on slow, deep inspiration. Diaphragm fluoroscopy is positive in more than 90% of patients with unilateral phrenic nerve paralysis. See Table 78.1 for a summary of fluoroscopic findings in the various conditions.
| Condition | Deep Inspiration | Sniffing | Ancillary Findings |
|---|---|---|---|
| Normal | Downward motion > 1 rib interspace | Usually downward motion | Occasional transient upward motion of right anterior hemidiaphragm during strong sniffing |
| Unilateral weakness | Downward motion < 1 rib interspace | May be upward or downward | Weakness more evident on rapid deep inspiration with weak hemidiaphragm lagging behind normal side |
| Unilateral paralysis | Absent downward motion or upward motion | Usually upward motion | Adjacent basal atelectasis; ipsilateral crus thinning on CT |
| Bilateral paralysis | Absent downward motion or bilateral upward motion | Usually upward motion | Adjacent basal atelectasis; supine imaging necessary to show absent motion; bilateral crus thinning on CT |
| Eventration | Reduced downward motion of affected segment; occasional upward motion | Downward or upward motion of segment | Normal ipsilateral crus thickness on CT |
Computed Tomography
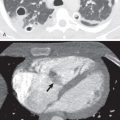
An important role of computed tomography (CT) in the assessment of patients with diaphragmatic paralysis is to rule out tumor, lymphadenopathy, aneurysm, or other lesion that may be compromising the phrenic nerve ( Fig. 78.3 ). The main role of CT in patients with eventration is in distinguishing the abnormality from a focal bulge along the diaphragm that might represent hernia or even tumor. In eventration the diaphragm, although thin, remains visible as a continuous layer over the elevated abdominal viscera and retroperitoneal or omental fat. There is often a sharp transition and undercutting at the edges of an eventration ( Fig. 78.4 ).


CT also is important in assessing the thickness of diaphragm muscle. The easiest place to observe muscle thickness is the crus of the hemidiaphragm. The left crus is normally slightly thinner than the right. The crus atrophies with paralysis but not with eventration ( Fig. 78.5 ). Thus the finding of an elevated hemidiaphragm with normal thickness of the crus likely reflects eventration rather than paralysis. If both hemidiaphragms are elevated, but the thicknesses of the crura are preserved, bilateral paralysis is unlikely, and some cause of abdominal distension, such as mass, ascites, or excess fat, is more likely.

Magnetic Resonance Imaging
Normal and abnormal diaphragmatic motion and diaphragmatic paralysis can be assessed with dynamic MRI. The advantage of MRI is avoiding ionizing radiation, as well as screening for central thoracic tumors that could be invading the phrenic nerve, but its disadvantages are high cost and lack of widespread availability.
Ultrasonography
Normal and abnormal diaphragmatic motion and diaphragmatic paralysis can be assessed with ultrasonography, which is often preferred for examination in children and young adults. At ultrasonography the diaphragm appears as a thick echogenic line. M-mode ultrasound is used to measure diaphragmatic motion, and interpretation is similar to that used in fluoroscopy. A paralyzed hemidiaphragm will lack downward motion on inspiration and may have paradoxical motion on sniffing. In fact, the ability of ultrasonography to assess diaphragmatic thickness and changing thickness with respiration is a potential advantage over fluoroscopy. Ultrasonography can be used in intubated patients to detect diaphragmatic thinning, which can influence weaning the patient from the ventilator.
Treatment
Conservative management is indicated for asymptomatic patients with hemidiaphragmatic weakness or paralysis. Diaphragmatic plication is usually reserved for symptomatic patients with irreversible unilateral phrenic nerve dysfunction or large eventration. Prophylactic diaphragmatic plication may also be beneficial in patients with phrenic nerve involvement by lung cancer or if phrenic nerve injury is recognized during surgery on the heart, mediastinum, or lung. Phrenic nerve stimulation may benefit patients with intact phrenic nerve function and absence of myopathy, such as those with high cervical spine injuries causing bilateral hemidiaphragmatic paralysis.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


