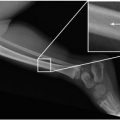
8-year-old female who fell on outstretched hands

1. What type of fracture is seen?
2. Which bone is most commonly affected in this entity?
3. What is the mechanism contributing to this entity?
4. Describe the findings that may present in this entity.
5. What are the treatment options?
Buckle fracture 83
Case ranking/difficulty: | Category: Upper extremities |
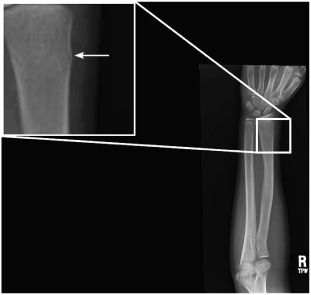
Frontal radiograph of the right forearm shows outward bulging of the lateral aspect of the distal radial cortex (arrow).

Lateral radiograph of the right forearm shows outward bulging of the anterior aspect of the distal radial cortex (arrow).
Answers
1. The diagnosis is Torus fracture (or Buckle fracture).
2. The most common bone affected in this entity is the distal radius.
3. The mechanisms contributing to this entity include axial loading, compression forces, fall on outstretched hands, and hyperextension.
4. The findings may include unilateral outward bulging of the bony cortex, bulging of the bony cortex in either end of the metaphysis, inward bulging with angulation of the bony cortex, or only inward bulging.
5. Casting is the only treatment for noncomplicated Buckle fracture.
Suggested Readings
Bozentka DJ, Beredjiklian PK, Westawski D, Steinberg DR. Digital radiographs in the assessment of distal radius fracture parameters. Clin Orthop Relat Res. 2002;397:409-413.
Reed MH. Fractures and dislocations of the extremities in children. J Trauma. 1977;17:351-354.
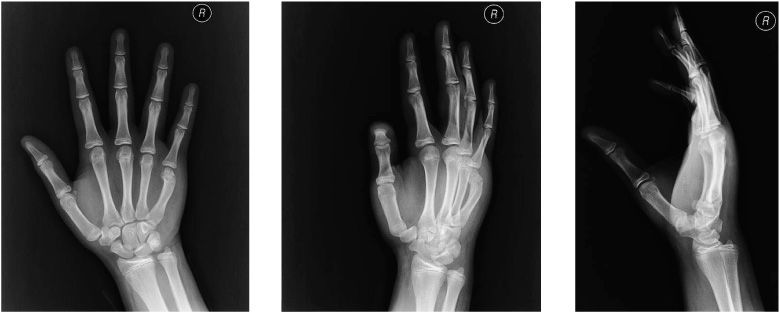
13-year-old male who punched his hand on an object
1. What is the finding?
2. What metacarpals may be involved in this entity?
3. What is the mechanism that contributes to this case?
4. In what direction does the apex of the angulation of the case point to?
5. What are the other names for this fracture?
Boxer’s fracture 129
Case ranking/difficulty: | Category: Upper extremities |

Frontal radiograph of the right wrist reveals fracture of the fifth metacarpal neck with apex ulnar angulation (arrow).

Oblique radiograph of the right wrist reveals fracture of the fifth metacarpal neck with apex ulnar angulation (arrow).

Lateral radiograph of the right wrist reveals fracture of the fifth metacarpal neck with apex dorsal angulation (arrow).
Answers
1. Fracture of fifth metacarpal neck called Boxer’s fracture.
2. The fifth or fourth metacarpals may be involved in Boxer’s fracture.
3. Striking a solid object with a clenched fist can lead to Boxer’s fracture.
4. The apex of the angulation in Boxer’s fracture is usually ulnar and dorsal.
5. Brawler’s fracture and bar room fracture.
Suggested Readings
Ashkenaze DM, Ruby LK. Metacarpal fractures and dislocations. Orthop Clin North Am. 1992;23(1):19-33.
Cornwall R. Finger metacarpal fractures and dislocations in children. Hand Clin. 2006;22(1):1-10.
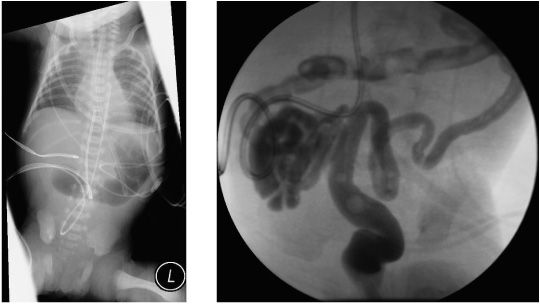
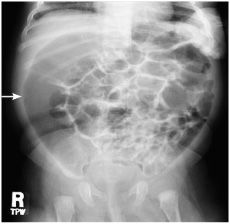
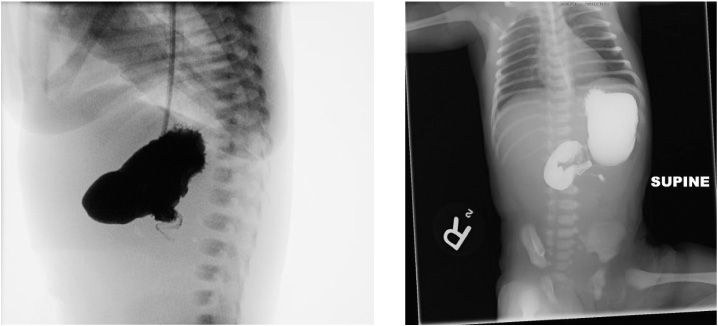
1-day-old male with failure to pass meconium
1. What are the findings?
2. What is the etiology of this entity?
3. What may cause this entity?
4. What are the entities that may be associated with the case?
5. What is the most commonly required treatment?
Microcolon 138
Case ranking/difficulty: | Category: Gastrointestinal |
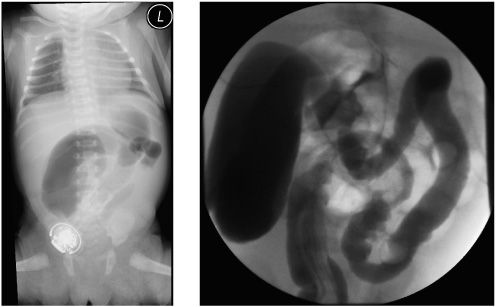
Frontal radiograph of the chest and abdomen reveals air in the stomach (black arrow) and air in the proximal duodenum (white arrow). Otherwise, the abdomen is gasless and no air is seen distally.

Water-soluble contrast enema reveals a colon small in caliber. Reflux to the distal ileum noted (asterisk).
Answers
1. The colon is noted to be small in caliber, consistent with the microcolon.
2. The etiology is congenital.
3. Microcolon is caused by a non-used colon during the fetal life. Reasons can be: ileal atresia, jejunal atresia, total colonic aganglionosis, meconium plug ileus, and cystic fibrosis that can lead to meconium ileus.
4. The entity shown is associated with cystic fibrosis. Also, it can be associated with megacystis-microcolon-intestinal hypoperistalsis syndrome.
5. Most commonly surgery is required, depending on the etiology.
Suggested Readings
LeQuesne G, Reilly B. Functional immaturity of the large bowel in the newborn infant. Radiol Clin North Am. 1975;13:331-342.
Loening-Baucke V, Kimura K. Failure to pass meconium: diagnosing neonatal intestinal obstruction. Am Fam Physician. 1999;60(7):2043-2050.
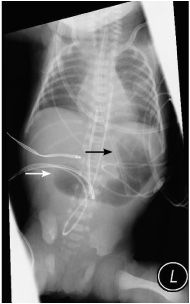
1-day-old male with abdominal distension
1. Describe the findings.
2. What are the predisposing factors of the case?
3. What is the presumed pathophysiology of the case?
4. What are the clinical symptoms?
5. What are the treatment options?
Neonatal small left colon syndrome 667
Case ranking/difficulty: | Category: Gastrointestinal |
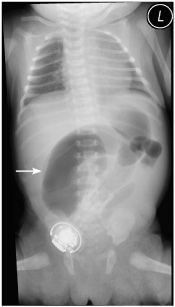
Frontal abdominal radiograph shows a dilated loop of bowel suggestive of obstruction (arrow).
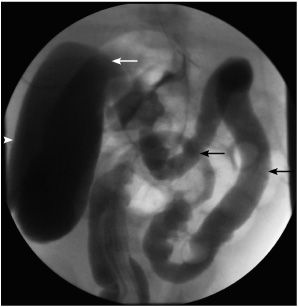
Fluoroscopic contrast enema demonstrates narrowed left and transverse colon (black arrows) with significantly dilated right colon (arrowhead). Transitional zone is noted in the region of the hepatic flexure (white arrow).
Answers
1. In the plain abdominal radiograph, a loop of bowel appears dilated suggestive of obstruction. The contrast enema demonstrates that the left colon and the transverse colon are small when compared to the dilated right colon. Transitional zone is noted at the level of the hepatic flexure.
2. Predisposing factors for neonatal small left colon syndrome include a diabetic mother, cystic fibrosis with development of meconium plug, hypermagnesemia, and aganglionosis of the entire left colon (Hirshprung’s disease).
3. The presumed pathophysiology of the case is neurohumoral imbalance between the autonomic nervous system and glucagon.
4. All patients do not pass meconium within the first 24 hours of life, and they all develop abdominal distension with bilious vomiting or nasogastric aspirates.
5. Treatment varies depending on the etiology. Initially repeats of enema relieve obstruction from meconium plug (if exists). Later, the treatment depends on the etiology. Cystic fibrosis requires medical management, while Hirshprung’s disease requires surgical intervention.
Suggested Readings
Berdon WE, Slovis TL, Campbell JB, et al. Neonatal small left colon syndrome: its relationship to aganglionosis and meconium plug syndrome. Radiology. 1977;125(2):457-462.
Ellerbroek C, Smith WL. Neonatal small left colon in an infant with cystic fibrosis. Pediatr Radiol. 1986;16(2):162-163.
Stewart DR, Nixon GW, Johnson DG, Condon VR. Neonatal small left colon syndrome. Ann Surg. 1977;186(6):741-745.
2-month-old male with constipation
1. What are the findings?
2. What is the diagnosis?
3. What are few of the differential diagnoses of this case?
4. What are diseases associated with this entity?
5. What are the treatment options?
Hirshprung’s disease 217
Case ranking/difficulty: | Category: Gastrointestinal |
Frontal radiograph of the abdomen reveals dilated colon filled with air (arrow).
Lateral view of a contrast enema reveals that the rectosigmoid ratio is less than one. Transitional zone is noted (arrows).
Answers
1. The plain frontal radiograph reveals dilated air-filled colon.
Contrast enema: Lateral view of the first pass of the rectal contrast in the recto-sigmoid area reveals that the diameter ratio of the rectum to the sigmoid is less than one. There is transitional zone. Proximal to the transitional zone, the sigmoid and the left colon are dilated. Distal to the transitional zone, the rectum is narrowed.
2. The diagnosis is Hirshprung’s disease.
3. Few of the differential diagnoses include constipation, hypothyroidism, and megacolon.
4. Among the diseases associated with Hirshprung’s disease are Down syndrome, neurocristopathy syndromes, multiple endocrine neoplasia type II, Waardenburg-Shah syndrome, and congenital central hypoventilation syndrome.
5. Treatment includes surgical resection of the abnormal section of the colon and reanastomosis.
Suggested Readings
Heanue TA, Pachnis V. Enteric nervous system development and Hirschsprung’s disease: advances in genetic and stem cell studies. Nat Rev Neurosci. 2007;8(6):466-479.
Russell MB, Russell CA, Niebuhr E. An epidemiological study of Hirschsprung’s disease and additional anomalies. Acta Paediatr. 1994;83(1):68-71.
Ryan ET, Ecker JL, Christakis NA, Folkman J. Hirschsprung’s disease: associated abnormalities and demography. J Pediatr Surg. 1992;27(1):76-81.
3-month-old female with upper GI study obtained to rule out gastroesophageal reflux
1. What are the findings?
2. Where is the normal anatomic location of the ligament of Treitz?
3. What is the normal relation between the superior mesenteric artery (SMA) and the superior mesenteric vein (SMV)?
4. What is the major risk of intestinal malrotation?
5. What is the treatment option?
Intestinal malrotation 68
Case ranking/difficulty: | Category: Gastrointestinal |
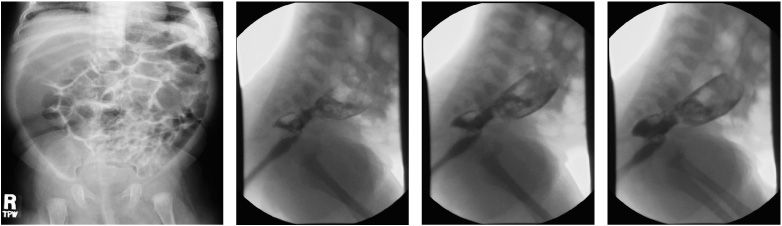
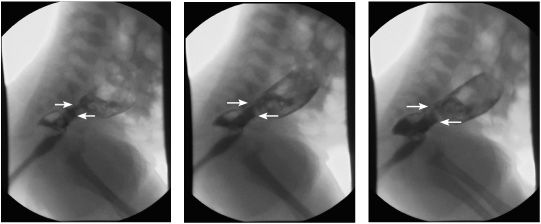
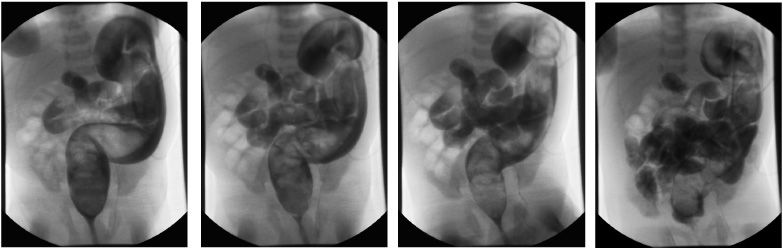
Early image of an upper GI study demonstrates the second portion of the duodenum in the right side of the abdomen, extending upwards (arrow). Normally, the second portion of the duodenum extends in the right abdomen downwards. The asterisk represents the stomach.
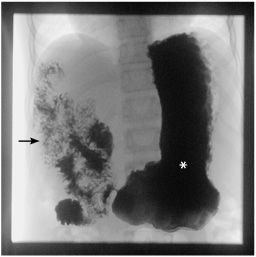
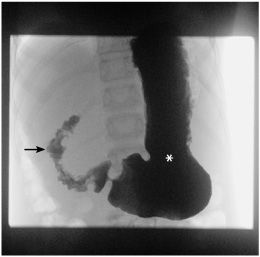
Late image of an upper GI study demonstrates the entire duodenum in the right side of the abdomen (arrow). The normal C-loop of the duodenum did not form. The duodenum did not cross the midline to the left. The ligament of Treitz is in the right upper quadrant of the abdomen. The asterisk represents the stomach.

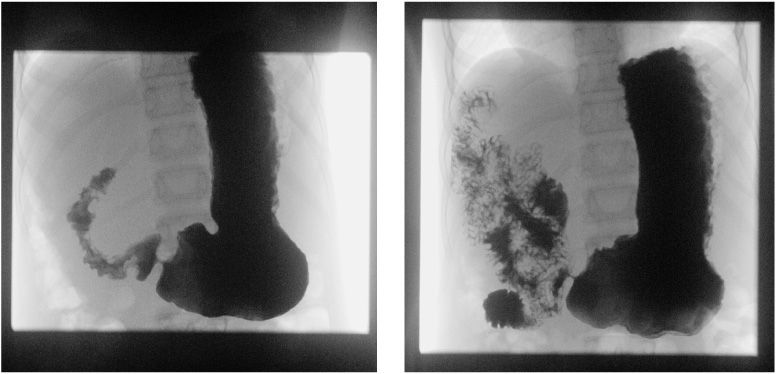
Normal upper GI study. C-loop of the duodenum is formed. The duodenum crossed the midline to the left. The ligament of Treitz (junction between the fourth portion of the duodenum and proximal jejunum) noted to be in its normal position, left of the spine and same level of the duodenal bulb. The asterisk points to the ligament of Treitz.
Answers
1. The diagnosis is intestinal malrotation. The C-loop of the duodenum did not cross midline to the left, and the ligament of Treitz is in the right upper quadrant of the abdomen.
2. The normal position of the ligament of Treitz is left of the spine and at the same level of the duodenal bulb.
3. Normally SMA is on the left side of SMV.
4. The major risk of intestinal malrotation is development of midgut volvulus.
5. Surgical treatment of malrotation consists of placement and fixation of small bowel on the right side of the abdomen and the large bowel on the left side of the abdomen. This is known as Ladd’s procedure.
Suggested Readings
Draus JM Jr, Foley DS, Bond SJ. Laparoscopic Ladd procedure: a minimally invasive approach to malrotation without midgut volvulus. Am Surg. 2007;73(7):693-696.
Estrada RL. Anomalies of Intestinal Rotation and Fixation. Springfield, IL: Charles C Thomas; 1958.
Irish MS, Pearl RH, Caty MG, Glick PL. The approach to common abdominal diagnosis in infants and children. Pediatr Clin North Am. 1998;45(4):729-772.
17-day-old female with history of gastroschisis repair with silo
1. How many degrees of normal intestinal rotation occur during the embryonic life?
2. What are the conditions associated with the case?
3. Around which vessel the normal intestinal rotation occurs during the embryonic life?
4. What is the differential diagnosis of the enema shown in this case?
5. What are the treatment options of gastroschisis?
Intestinal nonrotation 714
Case ranking/difficulty: | Category: Gastrointestinal |
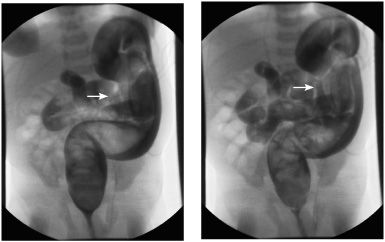
Fluoroscopic enema performed with water-soluble contrast demonstrates the entire colon in the left hemi-abdomen and the small bowel in the right hemi-abdomen. The arrow points to the distal ileum.
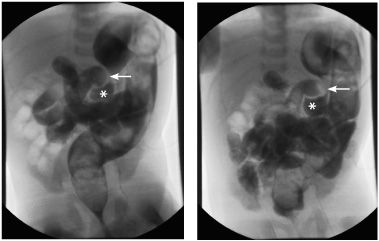
Fluoroscopic enema performed with water-soluble contrast demonstrates the entire colon in the left hemi-abdomen and the small bowel in the right hemi-abdomen. The arrow points to the distal ileum. The asterisk points the cecum.
Answers
1. The normal intestinal rotation during the embryonic life is 270 degrees counterclockwise.
2. Most infants with gastroschisis, omphalocele, or congenital diaphragmatic hernia present with intestinal malrotation. Intestinal malrotation occurs in association with Hirschsprung’s disease, persistent cloaca, imperforate anus, duodenal atresia, and extrahepatic anomalies.
3. Normal intestinal rotation takes place around the superior mesenteric artery.
4. Differential diagnosis of the shown enema includes Hirschsprung’s disease, intestinal nonrotation, colonic stricture, and bowel obstruction.
5. After birth, the lower body will be placed in a sterile bag to prevent infection in the exposed intestines. A silo, a special kind of sac, is wrapped around the intestines, holding them above the abdomen. Over the course of a week or more, the effects of gravity gently push most of the intestines into the abdominal cavity. When the intestines are level with the abdomen, surgery will be used to place the remainder of the intestines in the abdomen and close the opening. Surgical fixation of the bowel in the abdomen is performed in cases of malrotation or nonrotation.
Suggested Readings
Ford KL 3rd. Aunt Minnie’s corner. Nonrotation of the bowel. J Comput Assist Tomogr. 1997 Apr;20(4):693.
McLennan MK. Radiology rounds. Malrotation of the midgut with a nonrotation pattern. Can Fam Physician. 1998;44(44):271, 277-279.
3-day-old male with bilious vomiting
1. What is the clinical presentation of this case?
2. What is the risk factor of this entity?
3. What is the radiographic appearance of this case?
4. What is the age range that this condition is most commonly seen?
5. Why is the surgical treatment urgent?
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


