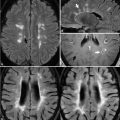
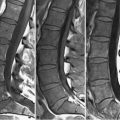
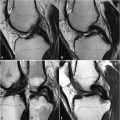
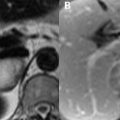
96 Diseases of Marrow The rationale for the SI characteristics of normal adult bone marrow on SE and FSE T1 and T2WI has been described in previous chapters. Marrow SI on MRI must be interpreted in the context of a patient’s age. At birth, hematologically active red marrow is widespread, its higher water content yielding a lower SI appearance than fatty marrow on T1WI. In the infantile stage of marrow development, fatty replacement begins at the phalanges, apophyses, and epiphyses. From that point on, fatty replacement progresses proximally, ending in complete replacement within the appendicular skeleton and a predominance of yellow over red marrow in the axial skeleton. Diffuse reconversion of yellow to red marrow may occur in pathologic conditions and normally in some individuals. The latter is erythropoietin-mediated and often present in endurance athletes and obese smokers, with a female predilection overall. Reconversion typically proceeds from the axial skeleton, where some residual hematopoietic marrow normally remains, to the appendicular system. Pathologic conditions leading to marrow hypointensity on T1WI include disorders leading to proliferation of cell line precursors such as leukemia, multiple myeloma, or polycythemia vera. The latter may progress to myelofibrosis, which appears as hypointensity on both T1WI and T2WI. Use of erythro- and granulocyte-stimulating chemotherapeutic agents may result in a similar appearance. The most common cause of hematogenous marrow reconversion is chronic anemia such as thalassemia or sickle cell. A case of the latter is illustrated in Fig. 96.1A
![]()
Stay updated, free articles. Join our Telegram channel



Full access? Get Clinical Tree


