Disorders of the Ankle and Foot
Forefoot
Technical Aspects
Doppler imaging has a crucial role in musculoskeletal ultrasound, allowing a real-time evaluation of regional blood flow, which may be altered in a variety of pathological conditions, including inflammation, infection and tumours. Doppler imaging also has an increasingly important role in the follow-up imaging, to assess therapeutic response. In general, power Doppler is preferred over colour Doppler for musculoskeletal ultrasound, as the former is subject to less background noise, is not affected by aliasing and is independent of the angle of insonation.
Trauma
Foreign Body
Imaging
The position of the foreign body in relation to other structures should be assessed, as should its size and depth beneath the skin. If an organic foreign body such as a thorn enters a joint or tendon sheath this may elicit a foreign body synovitis or tenosynovitis. Ultrasound can be used to mark the position of a foreign body prior to surgical removal or to guide minimally invasive removal using microforceps (Figs 28.1 and 28.2).
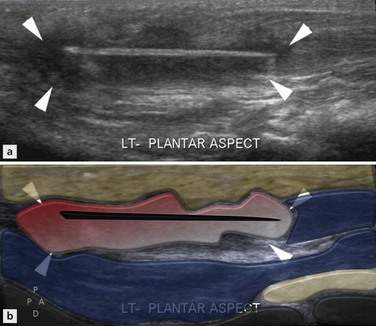
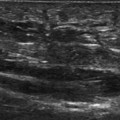
Figure 28.1 Wood splinter. Extended field of view image demonstrating a clearly defined linear echogenic foreign body in the sole of the foot with surrounding foreign body granuloma (arrowheads).
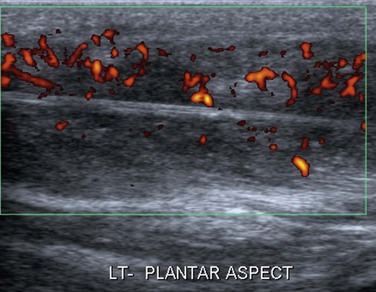
Figure 28.2 Wood splinter (same patient as in Figure 28.1). Power Doppler demonstrates marked increased vascularity within the foreign body granuloma.
Stress Fracture
Imaging
On ultrasound an acute stress fracture appears as a focal area of cortical disruption with associated hypoechoic haematoma and periosteal elevation. There is usually increased Doppler signal around the periosteal lesion. If a suspected stress fracture is seen it is prudent to obtain plain radiographs to confirm the lesion and act as a baseline (Fig. 28.3).
Plantar Plate Injury
Anatomy and Imaging
The plantar plate is a fibrocartilaginous supporting structure that connects the base of the proximal phalanx to the metatarsal neck, blending in with the sesamoids and tendons of the flexor hallucis brevis. Its function is to resist hyperextension of the MTPJ.
The plantar plate is best visualized in the longitudinal plane, and appears as a low-echogenicity band, curving over the metatarsal head to insert into the proximal phalanx.
The fibres of the plantar plate have a grainy homogeneous texture. Tears manifest as discontinuity of the plate or altered echogenicity (Fig. 28.4). There may be associated synovitis of the MTPJ, flexor tenosynovitis and persistent hyperextension of the proximal phalanx. If MRI is performed bone oedema may be seen in the metatarsal head and proximal phalanx due to hyperextension of the joint (Fig. 28.5).
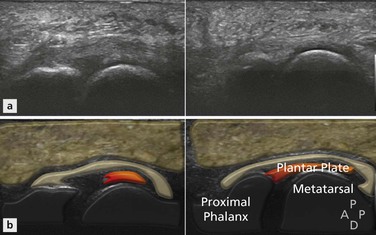
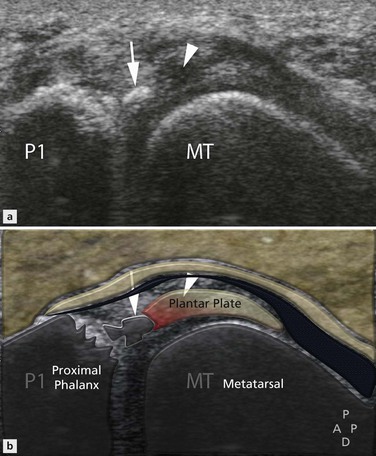
Figure 28.5 Turf toe. Longitudinal scan showing an avulsion of the base of the proximal phalanx (arrow) with discontinuity of the fibres of the plantar plate (arrowhead).
Sesamoiditis
Imaging
The hallux sesamoids are embedded within the medial and lateral slips of the flexor hallucis brevis tendon at the level of the first metatarsal head. A thick intersesamoid ligament connects the sesamoids, which in turn are attached to the base of the proximal phalanx by the sesamoid-phalangeal ligament. The anatomical arrangement forms part of a gliding mechanism that reduces friction and protects the tendon. A primary function of the hallux sesamoids is to absorb the weight-bearing force of the medial forefoot.
Plain radiographs should be obtained to assess for sclerosis or fragmentation of the sesamoids. In nearly all cases of sesamoiditis, the sesamoid bone is bi- or multipartite. On MRI there may be bony fragmentation with bone oedema on fluid-sensitive sequences. If there is avascular necrosis the affected sesamoid is of low signal on all sequences. Ultrasound may show fragmentation of the sesamoids, and in some cases there may be associated tendinopathy of the flexor hallucis longus tendon. Bipartite sesamoids can be difficult to differentiate from sesamoid fractures and most may even be fractures. Acute fractures have sharp, uncorticated margins, but this cannot usually be appreciated on ultrasound (Fig. 28.6).
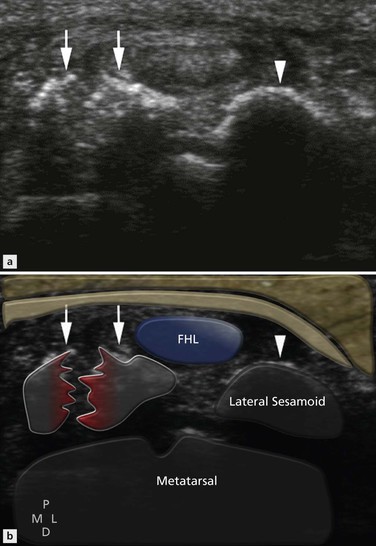
Figure 28.6 Sesamoiditis. Transverse scan showing a bipartite irregular medial sesamoid (arrows), with a normal appearance of the lateral sesamoid (arrowhead).
Freiberg’s Infraction
Imaging
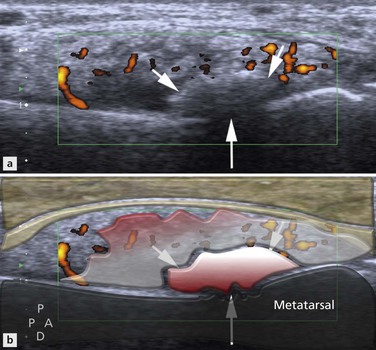
On radiographs there is initially sclerosis of the metatarsal head, followed by collapse and irregularity. On ultrasound the metatarsal head is flattened and irregular. There is often synovitis at the MTPJ, which may be associated with increased vascularity on Doppler (Fig. 28.7).
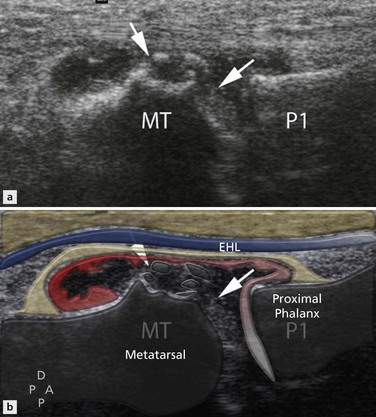
Figure 28.7 Freiberg’s infraction. Longitudinal scan showing irregularity of the second metatarsal head (arrows) with associated synovitis.
Masses
Ultrasound is often the first imaging modality used in the evaluation of soft-tissue masses. It allows a quick and effective means of confirming the presence of a lesion, and provides valuable information on the site, size, morphology and anatomical relations. Ultrasound can readily determine the cystic nature of ganglia, synovial cysts and bursitis. The location of the lesion in the foot can help narrow the diagnosis. For example, lesions between the metatarsal heads are almost invariably Morton’s neuromas or bursae.
Morton’s Neuroma
Imaging
The patient should be positioned supine on the couch with their foot in the neutral position. As described in Chapter 23, evaluation for Morton’s neuroma is best performed with the probe in the sagittal plane positioned either on the dorsum or plantar aspect of the forefoot. The forefoot is held steady with one hand while the probe is passed slowly across the MTPJ into the intermetatarsal space, and then across to the next MTPJ. When the probe is directly over the intermetatarsal space…
… it can be very helpful to press a finger into the dorsal aspect of the space to try to elicit symptoms and also improve the conspicuity of a suspected Morton’s neuroma.




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


