Table 19.1. The most dramatic improvement in the management of side effects was with the development of the 5-hydroxytryptamine antagonist antiemetics. More recently the Neurokinin-1 antagonist aprepitant has improved the emesis of patients undergoing cisplatin based chemotherapy. Typical antiemetic regimens are shown in
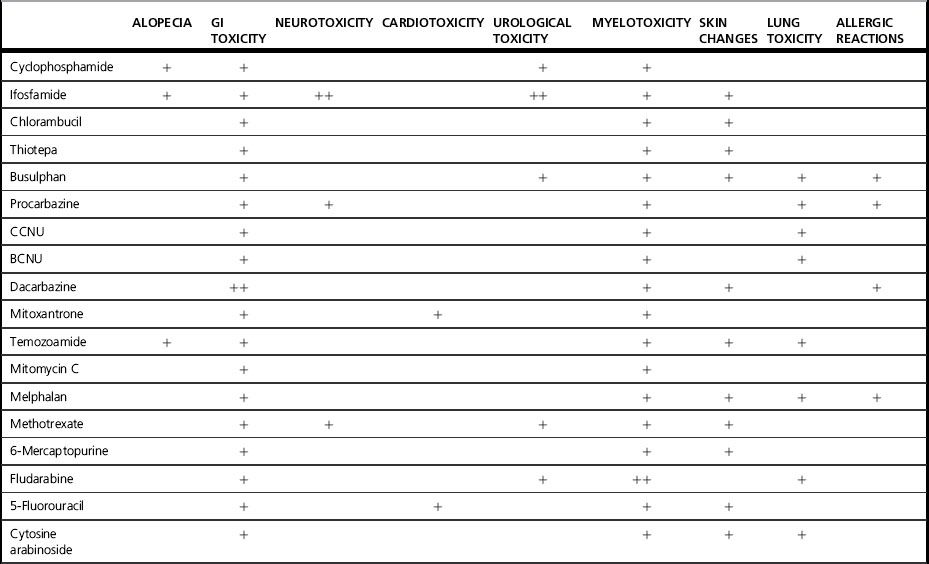
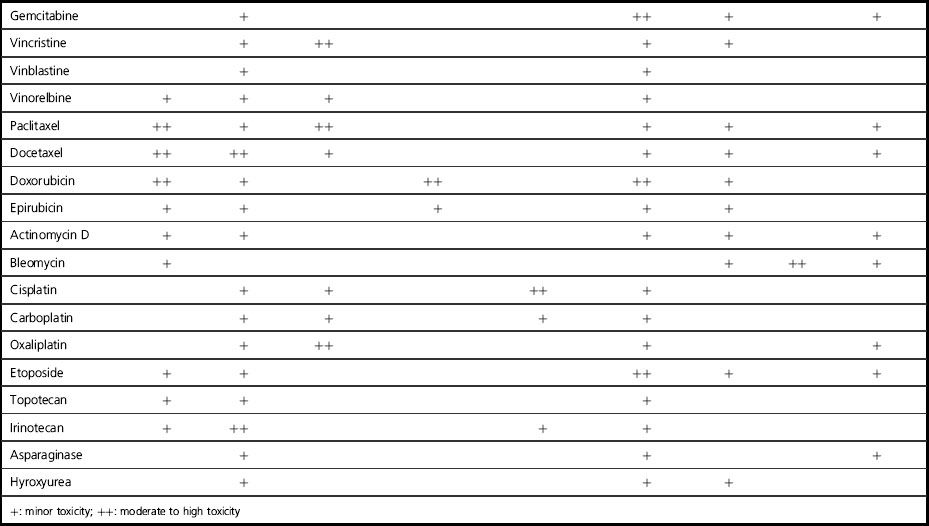
Table 19.2 Typical antiemetic regimens
| Grade of emesis | Antiemetic protocol |
|---|---|
| Low | Metoclopramide 20 mg IV if required Metoclopramide 10–20 mg orally (PO) tds PRN |
| Moderate | 5HT3 antagonist PO and dexamethasone 8 mg PO then Metoclopramide 20 mg tds Dexamethasone 4 mg bd Both for 3 days |
| High | 5HT3 antagonist PO and dexamethasone 8 mg PO then 5HT3 antagonist PO for 1 day Dexamethasone 4 mg bd for 3 days Metoclopramide 20 mg tds PRN |
| Second-line antiemetics | |
|---|---|
| Acute emesis | Give the antiemetic protocol for next grade of emesis |
| If already at ‘high’ give metoclopramide regularly, consider alternative antiemetics | Add in aprepitant 125 mg PO pre chemotherapy and 80 mg PO for 2 days post chemotherapy |
| Delayed emesis (>24 hours post chemotherapy) | Consider lengthening course of steroids, add in aprepitant and consider alternative antiemetics |
| Anxiety component | Add Lorazepam 1 mg PO or sublingually tds PRN. This can be started 1–2 days prior to chemotherapy |
| Alternative antiemetics | Domperidone rectally 30–60 mg 4–8 hourly PRN Haloperidol 1.5 mg tds PRN Cyclizine 50 mg tds PRN or regularly or levomepromazine 6 mg qds PRN |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


