Balloon
Company
Sheath size (Fr.)
Maximum balloon diameter (mm)
Catheter shaft length (cm)
Q-50
W.L.Gore
12
10–50
65
Coda
Cook, Inc. (Bloomington, IN, USA)
14
32, 40
100, 120
Reliant
Medtronic
12
46
100
Equalizer
Boston Scientific
65, 110
20, 27, 33, 40
65, 110
EVAR: If constant balloon inflation is required to maintain an adequate blood pressure then the contralateral limb is used to deliver the main body. The balloon is deflated and withdrawn immediately prior to stent graft deployment. Once the graft is deployed, if the blood pressure is such that it still requires balloon positioning, then it is delivered through the side of the main body and reinflated at the infrarenal aortic neck within the stent graft main body. The remaining EVAR is completed as per standard procedure (Chap. 22—Endovascular treatment of infra-renal aortic aneurysm).
An alternative to using the standard EVAR is the use of an aortouni iliac (AUI) device in circumstances such as inability to access the contra-lateral iliac artery (disease/tortuosity)
Assistive Procedures: These are required in cases where the anatomy might be less than ideal for EVAR. This includes but is not limited to:
1.
Hypogastric embolization for extension into the external iliac artery
2.
Use of chimney technique:
3.
Placement of a Palmaz stent proximally: Any sheath size larger than 16 Fr is adequate for delivering the stent. The Palmaz stent is centered on a 20–25-mm noncompliant Maxi LD balloon (Cordis, NJ, USA) and hand crimped. Holding the stent compressed the balloon is inflated so that the ends prevent “watermelon seed” displacement of the stent during deployment. The stent is delivered protected in the sheath upto the level of deployment, partly in the stent graft main body and partly in the native aortic neck. The sheath is then pulled back and the stent deployed. The deployment balloon is then exchanged for a compliant balloon so as to mold the Palmaz stent thus anchoring the stent graft to the aortic wall.
If the infrarenal neck is too short, too flared, or too angulated for an endovascular repair, open aortic repair is performed with the balloon being deflated only after proximal control has been established.
7 Benefits of Endovascular Repair (Fig. 17.1a–e)
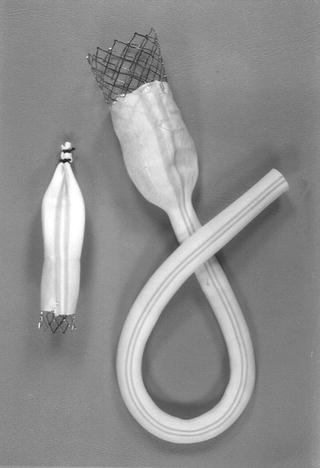
Fig. 17.1
Vascular Innovation (VI) graft. A large Palmaz stent is attached to the PTFE graft. A surgeon-made occluder device is shown on the left. However, there are many other commercially made occluders available, and any of these can be used to block the opposite common iliac artery
There are several advantages of endovascular repair of ruptured aneurysms.
7.1 Proximal Control Without General Anesthesia
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


