Entrapment neuropathies are a rare but presumably underdiagnosed cause of shoulder pain and painful instability. Radiologists must be aware of the clinical presentations and imaging features of these neuropathies because they may be the first to suggest these diagnoses. In this article, instead of a classical nerve-by-nerve approach, entrapment neuropathies are deciphered according to the clinical situation: which anatomic structures may be involved, how to explore them, which imaging abnormalities can be expected, how to manage differential diagnoses, and which therapeutic options can be considered.
Entrapment neuropathies are reported to be responsible for 2% of shoulder pain or painful instability. However, this frequency is likely to be underestimated because these conditions have been overlooked in the past. The main reasons for this are an ill-defined clinical presentation and a lack of specific clinical signs, whatever the nerve involved. The common feature is nerve damage, caused either by extrinsic compression or by stretching secondary to repeated movements. Electrodiagnostic studies are classically considered to be the gold standard for the diagnosis of entrapment neuropathies. However, the referring clinician must have considered this diagnosis to prescribe this test. Moreover, patients suffering from shoulder pain or weakness are often referred to the radiologist for a magnetic resonance (MR) examination. Because some lesional patterns are evocative of the diagnosis, the radiologist needs to know in what situations this diagnosis must be suggested, especially before concluding that the result of an MR imaging scan of the shoulder is normal.
To understand these conditions, and especially their imaging features, it is essential to recall some key anatomic points. The author then tackles the 2 different clinical situations a radiologist can encounter: either patients present with an abnormality of the position of the scapula, known as scapular winging, or they complain of nonspecific shoulder pain, which is the most frequent situation. After explaining the common imaging features, the distribution of the abnormalities proper to each type of nerve entrapment and their differential diagnoses are discussed.
Anatomic structures and landmarks
Suprascapular Nerve
The suprascapular nerve generally originates from the upper trunk of the brachial plexus, with fibers from the C5 and C6 nerve roots and partially the C4 nerve root. It runs posterolaterally from its origin and passes through the suprascapular notch ( Fig. 1 ). This notch, immediately medial to the root of the coracoid process, is highly variable in shape; 6 types have been reported ( Fig. 2 ). The transverse scapular ligament, which closes this notch, may be bifid and partially or completely ossified, and its thickness is variable. The suprascapular vessels also cross the superior edge of the scapula but remain above the suprascapular ligament.


Following its course in the posterior scapular region, the nerve passes under the supraspinatus muscle, which it innervates, and then through the spinoglenoid notch, situated between the root of the spine of the scapula and the glenoid cavity. This notch is inconsistently closed by the spinoglenoid ligament, which connects the scapular spine to the posterior glenohumeral capsule, turning the notch in a second osteofibrous tunnel. The suprascapular nerve terminates in and innervates the infraspinatus muscle.
The course of the nerve therefore presents 3 fixed points: the cervical origin, the suprascapular notch, and the spinoglenoid notch. The nerve also receives sensory branches from the glenohumeral and acromioclavicular joints and from the subacromial-deltoid bursa. Cadaver and clinical studies suggest that this nerve may be responsible for much of the sensation of the shoulder (up to 70%) and report that suprascapular nerve block is effective for the management of postoperative pain after shoulder surgery.
Axillary Nerve
The axillary nerve originates from the posterior cord of the brachial plexus, with fibers from the C5 and C6 nerve roots. It exits the axilla by passing through the quadrangular space together with the posterior circumflex humeral artery and vein. This space is limited superiorly by the inferior edge of the teres minor, inferiorly by the superior edge of the teres major, medially by the lateral edge of the long head of the triceps brachii, and laterally by the surgical neck of the humerus (see Fig. 1 A). Then the axillary nerve runs posterolaterally around the surgical neck of the humerus on the deep surface of the deltoid muscle. It provides motor innervation to the teres minor and deltoid muscles. It also has a cutaneous branch, which is sensory for the skin over the superior part of the deltoid muscle.
Long Thoracic Nerve
The long thoracic nerve arises from the C5 to C7 nerve roots. It runs downward, passing through the scalenus medius muscle. It descends behind the brachial plexus and the axillary vessels, resting on the outer surface of the serratus anterior muscle. It extends along the side of the thorax to the lower border of that muscle, supplying each of its digitations ( Fig. 3 ). Two fixed points are recognized: the scalenus medius muscle and the serratus anterior muscle at the level of the second rib.

Accessory Nerve
The accessory nerve, the eleventh cranial nerve, exits the skull through the nervous part of the jugular foramen. It descends obliquely in a posteroinferior direction and innervates the sternocleidomastoid and trapezius muscles from their deep surfaces, passing through the posterior triangle of the neck.
Dorsal Scapular Nerve
The dorsal scapular nerve arises from the brachial plexus, usually from the C5 root. It courses down posterior to the ribs and provides motor innervation to the rhomboid muscles and levator scapulae muscle.
Pathophysiology
Broadly speaking, nerves can be affected in 2 different situations: either by direct compression or by repeated microtrauma consecutive to particular movements (during sports or occupational activities).
Compressed Nerves
Direct compression occurs mainly because a space-occupying lesion develops in the vicinity of the nerve; this can also occur if the local anatomy has been modified by a fracture. The nerve is therefore affected by ischemic conditions, resulting in denervation lesions of the muscles, which it innervates. Any bony or soft tissue lesion can cause this. However, the most frequent situation is compression of the suprascapular nerve occurring at the suprascapular or spinoglenoid notch because of a cyst extending from the glenohumeral joint.
Nerve Stretching
There are fixed points along the course of each nerve, as described previously. Therefore, certain repetitive movements are thought to generate excess traction, thus entailing strain injuries at one or another of the fixed points. Inflammation occurs within the nerve, impairing its functioning. Additional elements, such as fibrous bands or small arterial branches crossing a nerve, can create additional fixed points. This can be responsible for an authentic entrapment situation ( Fig. 4 ). In the specific case of axillary neuropathy, entrapment occurs in the quadrilateral space, where fibrous bands linking the teres major and the long head of the triceps have been described. These points are not discussed because these structures cannot be precisely identified by imaging techniques.

Sensory impairment is responsible for pain and/or paresthesia, whereas motor impairment involves loss of strength and muscular atrophy. Multiple factors may be incriminated. In an overhead throwing position, the spinoglenoid ligament has been shown to tighten the suprascapular nerve, resulting in strain stress. Anatomic variants have also been reported to increase the risk of lesions; this is true for instances of variations in the morphology of the suprascapular notch (see Fig. 2 ). Another suggested mechanism of suprascapular neuropathy is arterial damage, leading to microemboli in the vasa nervorum and thus ischemic damage. Entrapment situations have been well described in overhead athletes and also in occupational situations, because repetitive movements are frequent in both situations.
Iatrogenic Lesions
Iatrogenic lesions (due to surgical procedures) can also be encountered. The accessory nerve may be injured after biopsies of the cervical lymph node. However, these situations are less diagnostically challenging and thus fall outside the scope of this discussion.
Pathophysiology
Broadly speaking, nerves can be affected in 2 different situations: either by direct compression or by repeated microtrauma consecutive to particular movements (during sports or occupational activities).
Compressed Nerves
Direct compression occurs mainly because a space-occupying lesion develops in the vicinity of the nerve; this can also occur if the local anatomy has been modified by a fracture. The nerve is therefore affected by ischemic conditions, resulting in denervation lesions of the muscles, which it innervates. Any bony or soft tissue lesion can cause this. However, the most frequent situation is compression of the suprascapular nerve occurring at the suprascapular or spinoglenoid notch because of a cyst extending from the glenohumeral joint.
Nerve Stretching
There are fixed points along the course of each nerve, as described previously. Therefore, certain repetitive movements are thought to generate excess traction, thus entailing strain injuries at one or another of the fixed points. Inflammation occurs within the nerve, impairing its functioning. Additional elements, such as fibrous bands or small arterial branches crossing a nerve, can create additional fixed points. This can be responsible for an authentic entrapment situation ( Fig. 4 ). In the specific case of axillary neuropathy, entrapment occurs in the quadrilateral space, where fibrous bands linking the teres major and the long head of the triceps have been described. These points are not discussed because these structures cannot be precisely identified by imaging techniques.
Sensory impairment is responsible for pain and/or paresthesia, whereas motor impairment involves loss of strength and muscular atrophy. Multiple factors may be incriminated. In an overhead throwing position, the spinoglenoid ligament has been shown to tighten the suprascapular nerve, resulting in strain stress. Anatomic variants have also been reported to increase the risk of lesions; this is true for instances of variations in the morphology of the suprascapular notch (see Fig. 2 ). Another suggested mechanism of suprascapular neuropathy is arterial damage, leading to microemboli in the vasa nervorum and thus ischemic damage. Entrapment situations have been well described in overhead athletes and also in occupational situations, because repetitive movements are frequent in both situations.
Iatrogenic Lesions
Iatrogenic lesions (due to surgical procedures) can also be encountered. The accessory nerve may be injured after biopsies of the cervical lymph node. However, these situations are less diagnostically challenging and thus fall outside the scope of this discussion.
Clinical presentation
The author has intentionally distinguished 2 different clinical presentations: the patient will present either with nonspecific shoulder pain or with a scapular prominence known as scapular winging. Although the latter presentation is more characteristic, it is far less frequent than that of shoulder pain associated with suprascapular or axillary nerve involvement.
These 2 situations must be distinguished by the radiologist because they require different MR imaging protocols. Although the sequences are the same, the field of view (FOV) needs to be adjusted. This adjusting is discussed later.
Nonspecific Shoulder Pain: Suprascapular and Axillary Nerve Entrapment
This condition is the most frequent situation in entrapment neuropathies of the shoulder. The supraspinatus, infraspinatus, or teres minor muscle is involved, thus mimicking other shoulder ailments, mainly tearing of the rotator cuff, and making for a difficult diagnosis.
Suprascapular neuropathy
Overhead athletes are typically affected by this disease, not only volleyball, baseball, handball, and tennis players but also swimmers. Patients usually complain of an insidious onset of dull aching pain in the superior or posterolateral aspects of the shoulder. Complaints of shoulder weakness and fatigue on exercise are common. Functional impairment is variable. At physical examination, infraspinatus or supraspinatus atrophy can be seen after several weeks. Functional impairment is possible, particularly in abduction and external rotation, depending on the level of compression; strength is more likely to be impaired in the case of proximal lesions (in regard to the infraspinatus and supraspinatus muscles) than that of distal lesions, where an isolated deficit of the infraspinatus muscle can be compensated by the surrounding muscles.
Axillary neuropathy: quadrilateral space syndrome
Axillary neuropathy affects young (25–35 years old) throwing athletes complaining of poorly localized anterolateral pain with paresthesia of the shoulder, overlying the deltoid muscle. Sustained flexion, abduction, and external rotation of the arm make the pain worse. On clinical examination, tenderness is found over the lateral aspect of the scapula, at the site of insertion of the teres minor.
Differential diagnosis: Parsonage-Turner syndrome
Also referred to as neuralgic amyotrophy or acute brachial neuritis, Parsonage-Turner syndrome is a rare (incidence estimated at 2–3 per 100,000 ) condition, characterized by sudden onset of shoulder pain associated with progressive weakness of the shoulder girdle muscles. The age of the patients varies widely, ranging from the third to the seventh decades. Men are predominantly affected, and a bilateral asymmetric presentation has been reported in up to one-third of the cases. Involvement of nerves outside the brachial plexus is reported in 17% of the patients. A history of recent viral infection, immunization, exercise, or surgery is sometimes reported. An autoimmune mechanism is suspected. The clinical symptoms are variable because patients present with isolated pain, weakness, or numbness or a combination of the 3, the most common presentations being associated pain and weakness followed by isolated pain. No asymptomatic presentation has been reported. However, the most typical presentation is an attack of severe relentless neuropathic pain involving 1 arm and worsening at night. The clinical diagnosis may be challenging because the symptoms are nonspecific and may mimic other shoulder girdle conditions such as labral tear, rotator cuff tear, impingement, and adhesive capsulitis.
Gaskin and Helms reported that the suprascapular nerve was almost invariably involved in patients with Parsonage-Turner syndrome (97% of cases); axillary nerve involvement was also commonly observed (in 50% of shoulders). However, any other nerve derived from the brachial plexus may be affected. The prognosis is poor, with 75% of the patients still experiencing pain and 25% still unable to work after 3 years, with a recurrence rate of 25% in the idiopathic form and 75% in the hereditary form of the condition.
Winging Scapula
On the other hand, entrapments of the long thoracic, accessory, or dorsal scapular nerves directly impede scapular movements because of the muscles involved. These entrapments are responsible for the static or dynamic scapular prominence known as scapular winging.
This clinical situation is different from suprascapular and axillary nerve entrapment because there is a clinical abnormality evocative of it, which can be detected on physical examination. The patient is likely to be referred for the exploration of this abnormality.
Long thoracic nerve neuropathy
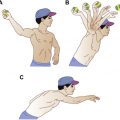
This condition is responsible for medial scapular winging, which is more frequent than the lateral form. The scapular asymmetry (objectivized by comparing the distance between the spinal processes and the medial edge of the scapula on both sides) may be clinically obvious on physical examination ( Fig. 5 A). It can be exacerbated still more on forward flexion of both arms (see Fig. 5 B) or by the wall push-up test. In the most severe cases, full elevation of the arm may be impossible.
Accessory nerve neuropathy
Lateral scapular winging is always present. However, it is only in the more severe forms that the droopy shoulder aspect may be seen, associating trapezius atrophy, shoulder drop, and lateral winging. Abduction and external rotation against resistance exacerbate the scapular displacement, whereas forward flexion lessens the deformation because of serratus anterior contraction. As described earlier, this nerve is wounded mainly because of biopsies of the cervical lymph node.
Dorsal scapular nerve neuropathy
Dorsal scapular nerve neuropathy is a very rare condition, responsible for levator scapulae and rhomboid muscle denervation. Pain in this area may be encountered and may be the only symptom. Mild scapular winging is encountered. The functional impact is negligible.
Imaging entrapment neuropathies
Identifying muscular denervation (muscular edema, atrophy, and fatty degeneration) in a neural distribution pattern is key to the diagnosis of entrapment neuropathies. The MR imaging protocol needs to be adapted to each situation: in case of suspected suprascapular or axillary entrapment, the FOV needs to be centered on the glenohumeral joint, whereas in case of scapular winging, the FOV has to be enlarged to include both scapulas, covering the posterior and medial muscles attaching to them. Apart from this difference, the semiology and reasoning are the same. In this article, the author successively discusses the prevailing role of MR imaging among other imaging modalities, the MR imaging protocol required for each clinical situation, the abnormalities to be sought, and the systematic analysis to be performed when exploring these conditions.
Imaging Modalities: the Prevalent Role of MR Imaging
The author focuses on MR imaging because it is the only imaging modality that allows the detection of muscular edema, which is the earliest abnormality to appear. MR imaging also allows an evaluation of the severity of the disease and the search for a cause. It is also very efficient in excluding several differential diagnoses. Once radiologists understand what to look for and how to do it in MR imaging, they will be able to reproduce this scheme with other imaging modalities, each of which has its own limitations.
Other imaging modalities perform less well. Plain radiographs are useful to appreciate the gross morphology of the scapula, especially the suprascapular notch, by using dedicated views. A fracture, an osteolytic lesion, or calcifications of the surrounding soft tissues can also be detected. Computed tomographic (CT) scan does the same job in a more accurate way and allows the identification of muscular fatty degeneration and atrophy. CT arthrography helps identify some paralabral cysts and differential diagnoses such as rotator cuff tears.
Shoulder ultrasonography (US) is not the best method for the exploration of these conditions because it cannot identify muscular edema. However, the technique’s role should not be neglected. It is routinely used as a first-intention modality for shoulder pain. Although the initially suspected diagnosis is often a rotator cuff tendon tear, the radiologist must not overlook differential diagnoses, especially when no cuff tendon abnormality has been identified. For this reason, we suggest that the reader systematically includes the following items in a US shoulder examination :
- •
The suprascapular and spinoglenoid notches, in search of a space-occupying lesion ( Fig. 6 ). A paralabral or mucoid cyst can be easily differentiated from dilated suprascapular veins by combining color Doppler and compression of the structure; veins are filled with colored flow signal and collapse under pressure, whereas cysts do not.
Related posts:
 Magnetic Resonance Imaging of Rotator Cuff Disease and External Impingement
Magnetic Resonance Imaging of Rotator Cuff Disease and External Impingement
 Internal Impingement Syndromes
Internal Impingement Syndromes
 The Throwing Shoulder: the Orthopedist Perspective
Postoperative Shoulder Magnetic Resonance Imaging
Magnetic Resonance Imaging of the Pediatric Shoulder
The Throwing Shoulder: the Orthopedist Perspective
Postoperative Shoulder Magnetic Resonance Imaging
Magnetic Resonance Imaging of the Pediatric Shoulder
 Anatomic Variants and Pitfalls of the Labrum, Glenoid Cartilage, and Glenohumeral Ligaments
Anatomic Variants and Pitfalls of the Labrum, Glenoid Cartilage, and Glenohumeral Ligaments

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


