Fig. 18.1
Lowest renal artery—right renal
These aneurysms are most commonly due to degenerative atherosclerotic disease.
Abdominal aortic aneurysms with short or absent infrarenal necks (less than 10–15 mm) are not suitable for treatment with standard “off-the-shelf” endoluminal devices, and prior to the advent of fenestrated stent grafts (FSG), open surgical repair has been the only treatment option. FSGs are so named because they incorporate holes or fenestrations in the graft fabric to allow for continued aortic branch perfusion (usually through stents), whilst achieving a haemostatic seal at the same aortic level.
3 Disease Prevalence
Juxtarenal aortic aneurysms account for approximately 15 % of abdominal aortic aneurysms. Unfavourable anatomy of the proximal aortic neck of an infrarenal abdominal aortic aneurysm is the cause in up to 40 % of the patients who are precluded from an endovascular option.
4 Diagnosis
4.1 Clinical
The diagnosis is usually made incidentally on imaging of the abdomen for other causes. If patients are symptomatic, they will present with abdominal pain or back pain with or without associated symptoms of shock.
4.2 Imaging
4.2.1 Ultrasound
Most abdominal aortic aneurysms are detected by ultrasound, an increasingly so as population screening becomes more widespread.
4.2.2 CT angiography
Assessing suitability for endovascular repair requires CT aortography. In cases where consideration is given to the use of a fenestrated device, thin slice (<3 mm, preferably <1 mm) CT is essential. Both the thoracic and abdominal aorta should be included as well as the iliac and common femoral arteries. Precise measurement of the distance between each visceral aortic branch and the radial position of these branches is required and 3-dimensional CT reconstruction software is essential for this purpose. This allows for a straightened view of the aorta (Fig. 18.2) orthogonal to the line that the proposed stent graft will be expected to take, which enables clear visualisation of the position of each target vessel relative to the proposed device. With currently available multi-detector row CT scanning machines and reconstruction software, further diagnostic imaging is rarely required for planning of treatment.
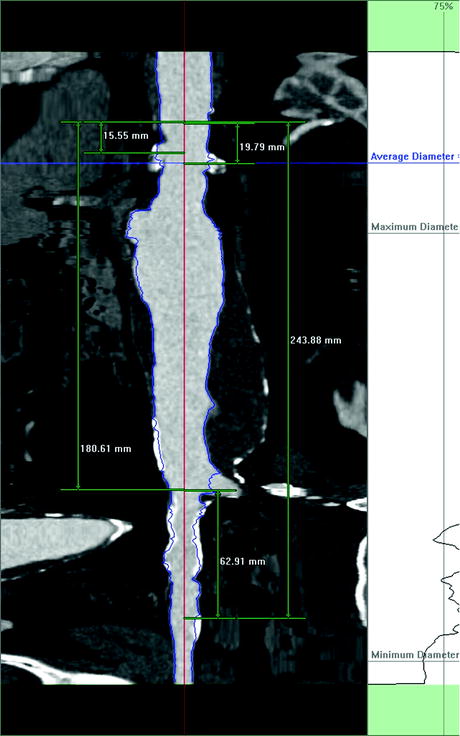
Fig. 18.2
Centerline of flow—straightened view of aorta
4.2.3 MR angiography
While adequate imaging is possible with MR angiography, but it is more time consuming.
4.2.4 Digital Subtraction Angiography (DSA)
This has largely been abandoned in favour of CT angiography. However it is occasionally used to supplement the information of the CTA.
5 Management
Open surgical repair must be considered for all patients who present with juxtarenal aneurysms, as this remains the gold standard for good risk patients. This will usually require a period of suprarenal clamping and may or may not require re-implantation of one or both renal arteries. Endovascular repair was initially offered to those deemed unfit for open surgery, but as acceptable early results have been reported, it is increasingly seen as an option for all patients.
Suitability for a fenestrated stent graft is determined largely by the anatomy of the aortic neck, and for the purpose of this discussion we assume acceptable access vessels and a standard anatomy of visceral arteries. The aortic level at which a haemostatic seal between the stent graft and healthy aorta can be achieved will determine the complexity of the endovascular repair required.
1.
Adequate infrarenal aneurysm neck: Standard EVAR
2.
Short (inadequate) infrarenal neck and healthy neck at the level of the renal arteries: A fenestrated stent graft with two small fenestrations for the renal arteries and a scallop for the SMA
3.
Absent infrarenal neck and healthy aorta at the renal arteries: Fenestrated SG as in 2, provided that there is sufficient distance between the renal arteries and the SMA to allow for an adequate haemostatic seal. In most cases where the aorta is aneurysmal at the level of the renal arteries it will be necessary to “climb higher” to achieve a seal zone by means of two small fenestrations for the renal arteries, a larger (strut free) fenestration for the SMA and a scallop for the coeliac trunk.
4.
Where the potential for a haemostatic seal zone only occurs at the level of the SMA or coeliac arteries, consideration is given to “triple” (as in 3 above) or even “quadruple” fenestrated stent grafts. The complexity of these procedures is considerable compared with the more standard “double fenestrated” cases (unpublished observations) and other options, particularly the use of thoracoabdominal branched devices (Chap. 19: Branched aortic endografts—thoracoabdominal aortic aneurysms), or of open surgical repair, must be considered.
6 Planning and Sizing
The only commercially available fenestrated stent graft is manufactured by Cook Medical (Perth, Australia) and so the steps for planning are in accordance with the specifications of this device.
1.
Inner aortic diameter at the level of the fenestrations will determine the diameter of the sealing stent (or stents, there is an option for 1 or 2 sealing stents in the fenestrated device).