Fetal Biometry and Pregnancy Dating in the First Trimester
INTRODUCTION
Accurate performance of an ultrasound examination in the first trimester is important given its ability to confirm an intrauterine gestation, assess number and viability of embryos or fetuses, accurately date the pregnancy, and diagnose major fetal malformations. In this chapter, we present the approach and indications to the first trimester ultrasound examination, the parameters of pregnancy dating, and the ultrasound markers of pregnancy failure. Normal fetal anatomy and fetal malformations will be discussed in detail in subsequent chapters.
APPROACH TO THE FIRST TRIMESTER ULTRASOUND EXAMINATION
The first trimester ultrasound examination can be performed transabdominally or transvaginally. There is general consensus that, with rare exceptions, obstetrical ultrasound examinations at less than 10 weeks of gestation are best performed transvaginally. The transvaginal approach provides for higher resolution than the transabdominal approach and positions the transducer in close proximity to the target anatomic region (gestational sac). Beyond the 12th week of gestation, the transabdominal approach with high-resolution transducers and with optimal imaging can provide sufficient details to allow for systemic assessment of fetal anatomy. In the presence of first trimester suspected fetal malformations, a combined transabdominal and transvaginal approach is recommended.
INDICATIONS FOR THE FIRST TRIMESTER ULTRASOUND EXAMINATION
There is currently varying opinions on whether the first trimester ultrasound examination is offered routinely to all pregnant women or is indication driven.1,2 Indications for the first trimester ultrasound are many and most pregnant women in resourced settings receive at least one such ultrasound during their pregnancies. With mounting evidence on the important role of the first trimester ultrasound in pregnancy dating, aneuploidy risk assessment, diagnosis of multiple pregnancies, and in detection of major fetal malformations, the authors believe that ultrasound in early gestation will ultimately be offered routinely to pregnant women. Table 4.1 lists common indications for the first trimester ultrasound examination in pregnancy.
SONOGRAPHIC LANDMARKS IN THE FIRST TRIMESTER
The normal intrauterine pregnancy undergoes significant and rapid change in the first trimester, from a collection of undifferentiated cells to a fetus within an amniotic sac connected to a placenta and a yolk sac. This significant progression can be seen on ultrasound beginning with the chorionic sac, which
is the first sonographic evidence of pregnancy and progressing to the embryo and fetus with cardiac activity. Identifying ultrasound landmarks and understanding its normal progression in the first trimester help in confirming a normal pregnancy and in the diagnosis of pregnancy failure.
is the first sonographic evidence of pregnancy and progressing to the embryo and fetus with cardiac activity. Identifying ultrasound landmarks and understanding its normal progression in the first trimester help in confirming a normal pregnancy and in the diagnosis of pregnancy failure.
Table 4.1 • Common Indications for Ultrasound examination in the First Trimester | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
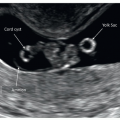
Gestational Sac
The gestational sac, also referred to as the chorionic cavity, is the first sonographic evidence of pregnancy. The gestational sac on transvaginal ultrasound is first seen at 4 to 4.5 weeks from the first day of the last menstrual period (LMP) (Fig. 4.1). When the gestational sac has a mean diameter of 2 to 4 mm, its borders appear echogenic, which makes its demonstration easy (Fig. 4.1). The echogenic ring of the gestational sac is an important ultrasound sign, which helps to differentiate it from intrauterine fluid or blood collection (Fig. 4.2). The shape of the gestational sac is first circular but with the appearance of the yolk sac and the embryo it becomes more ellipsoid (Fig. 4.3).
Yolk Sac
The yolk sac is seen at 5 weeks of gestation (menstrual age) on transvaginal ultrasound, as a small ring within the gestational sac with highly echogenic borders (Figs. 4.3 and 4.4). It has a diameter of around 2 mm at 6 weeks and increases slowly to around 6 mm at 12 weeks. The first detection of the embryo by ultrasound is noted in close proximity to the free wall of the yolk sac, because the yolk sac is connected to the embryo by the vitelline duct. A small yolk sac with a diameter less than 3 mm between 6 and 10 weeks or a diameter of more than 7 mm before 9 weeks is a cause for concern for an abnormal pregnancy and thus this observation requires a follow-up ultrasound examination to assess normalcy of pregnancy (Fig. 4.5A and B).
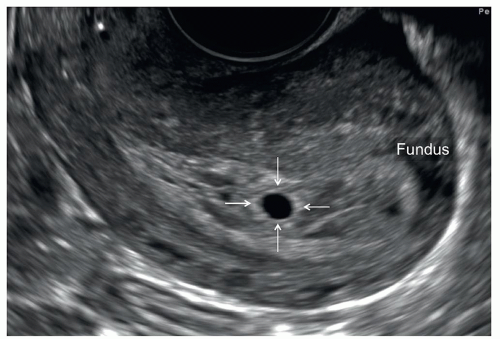 Figure 4.1: Midsagittal plane of a uterus with a gestational sac at 4.5 weeks of gestation. Note the echogenic borders (arrows) of the gestational sac. The echogenic borders (ring) of the gestational sac help to differentiate it from an intrauterine fluid or blood collection. The fundus of the uterus is labeled for orientation. |
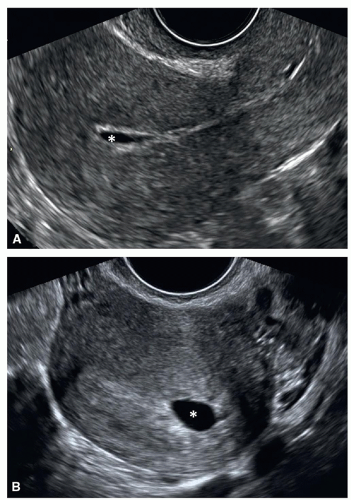 Figure 4.2: Midsagittal (A) and transverse (B) planes of two uteri showing fluid accumulation (asterisk) between the decidual layers. This finding should not be confused with an intrauterine gestational sac. See text for details. |
Amnion
The amniotic sac develops as a thin echogenic structure surrounding the embryo (Fig. 4.6). The amniotic sac appears following the appearance of the yolk sac and just before the appearance of the embryo. Whereas the gestational sac shows variations in size and shape, the growth of the amniotic sac is closely related to that of the embryo between 6 and 10 weeks of gestation.
Embryo
The embryo is first seen on transvaginal ultrasound as a focal thickening on top of the yolk sac, at around the fifth menstrual week (Fig. 4.7). First cardiac activity is typically seen by 6 to 6.5 weeks. The embryo can be recognized by high-resolution transvaginal ultrasound at the 2 to 3 mm length size (Fig. 4.7), but cardiac activity can be consistently seen when the embryo reaches a 5 to 7 mm in length or greater. Embryonic heart rate increases rapidly in early gestation being around 100 to 115 before 6 weeks, rising to 145 to 170 at 8 weeks, and dropping down to a plateau of 137 to 144 after 9 weeks of gestation.
The size of the embryo increases rapidly by approximately 1 mm per day in length. Note that the embryo develops within the amniotic cavity and is referred to as intraamniotic whereas the yolk sac is outside of the amniotic cavity and is referred to as extraamniotic. The fluid that the yolk sac in embedded within is the extraembryonic coelom.
The size of the embryo increases rapidly by approximately 1 mm per day in length. Note that the embryo develops within the amniotic cavity and is referred to as intraamniotic whereas the yolk sac is outside of the amniotic cavity and is referred to as extraamniotic. The fluid that the yolk sac in embedded within is the extraembryonic coelom.
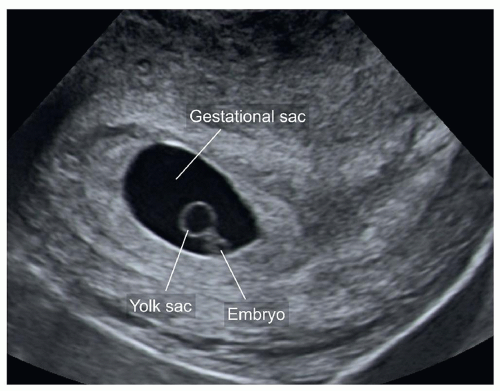 Figure 4.3: Midsagittal plane of a uterus with a gestational sac at 6 weeks of gestation. Note the presence of a yolk sac and a small embryo. The shape of the gestational sac is more ellipsoid than circular. |
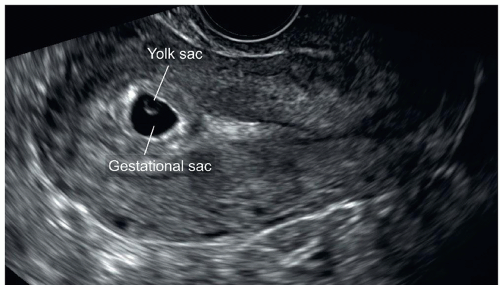 Figure 4.4: Midsagittal plane of a uterus with a gestational sac at 5.5 weeks of gestation. Note the yolk sac seen within the gestational sac with highly echogenic borders. |
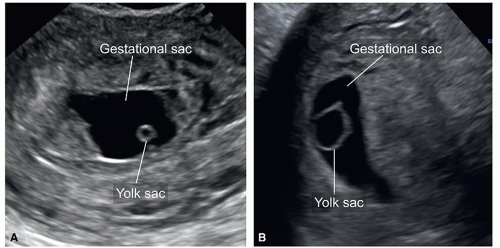 Figure 4.5: A and B: Two gestational sacs with abnormal size of yolk sacs: small in A and large in B. Abnormal size of yolk sacs is a concern for an abnormal pregnancy and follow-up ultrasound is recommended. |
The appearance of the embryo on ultrasound changes from 6 to 12 weeks of gestation. At 6 weeks of gestation, the embryo appears as a thin cylinder with no discernible body parts, “the grain of rice appearance” (Fig. 4.8). As gestational age advances, the embryo develops body curvature and clear delineation on ultrasound of a head, chest, abdomen, and extremities, “the gummy-bear appearance” (Figs. 4.9 and 4.10). Clear delineation of a head, chest, abdomen, and extremities on gray scale ultrasound is noted at 10 weeks of gestation and beyond (Fig. 4.11). Close observation of anatomic details on transvaginal ultrasound at or beyond 12 weeks of gestation may allow for the diagnosis of major fetal malformations. This will be discussed in detail in Chapters 8, 9, 10, 11, 12, 13 and 14, organized by anatomic organ system.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


