trimester when available and technically feasible, as this enables a detailed anatomic evaluation of the fetus in keeping with existing guidelines1,2 (see Chapter 1). In the first trimester, the use of high frequency transducers provides adequate imaging, thus allowing for optimal nuchal and intracranial translucency evaluation along with clear visualization of fetal organs such as brain, heart, lungs, stomach, kidneys, and bladder. The general contour of the fetus with the surrounding amniotic fluid can be imaged (Fig. 3.1A), in addition to the skeletal system to include the skull, nasal bone, ribs, spine, and limbs (Fig. 3.1A-E). Limitations of transabdominal high frequency transducers are encountered when the fetus is deep in the pelvis. Recently, linear transducers, that are commonly used for soft tissue imaging in radiology, have been adapted to obstetric imaging.3 These linear transducers are desirable because of their high resolution with good tissue penetration of sound. Unlike the curved array transducers, the linear transducers have ultrasound beams that are uniform throughout all tissue levels and do not diverge in deeper tissue. We have found linear transducers to be well adapted for first trimester ultrasound imaging and can provide detailed anatomic evaluation of the fetus (Fig. 3.2) with comparable resolution to that of transvaginal transducers.4
Table 3.1 • Image Optimization for Two-Dimensional Ultrasound in Gray Scale in the First Trimester | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
 Figure 3.1: Various planes (A-E) obtained by a transabdominal curved array high-resolution transducer in fetuses at 12 to 13 weeks of gestation. Plane A represents a midsagittal view of the fetus obtained for measurement of crown-rump length, nuchal and intracranial translucency, and for visualization of the nasal bone. Plane B is an axial view of the head. Plane C is a frontal facial view. Plane D shows two lower limbs and plane E represents the four-chamber view. |
between 10 and 12 weeks of gestation and embryos before 10 weeks of gestation are better imaged by the transvaginal approach. It has also been our experience that the NT and nasal bones are imaged easily with transabdominal transducers. Figures 3.5 and 3.6 display the fetal abdomen and face respectively with the transabdominal curvilinear, transabdominal linear, and transvaginal transducers. Note that the three transducers provide adequate imaging of upper abdominal structures (Fig. 3.5), whereas the linear and transvaginal transducers provide superior imaging for complex anatomic regions such as the facial profile (Fig. 3.6).
 Figure 3.2: Various planes (A-F) obtained by a transabdominal high-resolution linear transducer in fetuses at 12 to 13 weeks of gestation. Compare with Figure 3.1. Plane A represents a midsagittal view of the fetal head. Plane B is a frontal facial view. Plane C shows the intracerebral structures. Plane D shows a hand with digits. Planes E and F show a sagittal and coronal view of the fetal spine respectively with fetal kidneys noted in plane F. Note the high resolution of these images as compared to images in Figure 3.1. |
 Figure 3.3: A: A fetus at 12 weeks of gestation scanned transabdominally with color Doppler at the three-vessel trachea view. Note that the image displays decreased resolution, primarily due to the long distance between the transducer and the region of interest; upper fetal chest in this case (yellow arrow). Note also that the fetus is deep in the pelvis and near the cervix (white arrow). B: A transvaginal view showing that the fetus is in a transverse lie, an ideal fetal position for a transvaginal ultrasound examination. C: A transvaginal ultrasound in color Doppler at the three-vessel trachea view showing improved resolution over the transabdominal approach in A. Planes B and C are obtained in the same fetus as plane A. |
 Figure 3.4: Various planes (A-F) obtained by a transvaginal high-resolution transducer in fetuses at 11 to 13 weeks of gestation. Compare with Figures 3.1 and 3.2. Plane A represents a midsagittal view of the fetal head. Plane B shows the intracerebral structures. Plane C shows a midsagittal view of the spine. Plane D is a four-chamber view of the fetal heart. Plane E shows a fetal hand with digits and plane F is a coronal view of the chest and abdomen showing the fetal kidneys. Note the high resolution of these images as compared to images in Figures 3.1 and 3.2. |
obstacle as it provides various approaches to imaging within a relatively short time frame. Asking the mother to cough or to walk around for few minutes can often lead the fetus to move and change position. Furthermore, applying gentle pressure with the transducer during the transabdominal ultrasound examination may shorten the distance to the fetus and improves imaging. With the transvaginal approach, the transducer should be inserted gently into the vaginal canal, thus making the examination well tolerated by most women.5 Following the introduction of the transvaginal transducer, the operator should visualize the entire uterine cavity, including the fetus, without magnification. Following this overview, the region of interest can be magnified to optimize imaging and to get detailed anatomic assessment. Occasionally, a gentle manipulation of the uterus with the other hand placed on the maternal abdomen can lead to a change in the position of the fetus and brings the region of interest into the focus region.
 Figure 3.5: Axial views of the fetal abdomen at 12 weeks of gestation in three fetuses (A-C) using three different high-resolution transducers: A—transabdominal curved array, B—transabdominal linear, and C—transvaginal. Note the increased resolution in planes B and C. St, stomach. |
 Figure 3.6: Midsagittal views in three fetuses at 12 to 13 weeks of gestation, imaged with three different high-resolution transducers: A—transabdominal curved array, B—transabdominal linear, and C—transvaginal. Note the increase in resolution and tissue characterization in C as compared to A and B. Also note that the nasal bone (arrows) has sharp borders in B and C, as compared to blurred borders in A. When fetal malformations are suspected, the transvaginal approach provides more detailed assessment of fetal anatomy in early gestation. |
 Figure 3.7: A: An axial plane of the fetal chest at 13 weeks with the application of pulsed-wave Doppler on the heart to demonstrate and document cardiac activity. The authors do not recommend this practice given the increased energy associated with pulsed-wave Doppler. It is recommended to use M-mode or to save a gray scale movie clip for this purpose (see Chapter 2). When color Doppler is indicated, an application of the color box over the fetus (B) can document cardiac activity and demonstrate an intact anterior abdominal wall (arrow) and a normal course of the ductus venosus (DV). |
the ultrasound examination. Velocity scale or pulse repetition frequency is used to determine the range of mean velocities within the color box. For color Doppler interrogation of the cardiac chambers and the great vessels, a high velocity range (>30 cm per second) should be selected. For the examination of the umbilical arteries and veins, renal arteries, or other fetal peripheral vasculature, lower velocity ranges should be selected (5 to 20 cm per second). Table 3.2 summarizes the presets that we commonly use for color Doppler application in the first trimester. For a more comprehensive presentation on this subject, the readers are referred to our previous work on the optimization of the color Doppler ultrasound examination of the fetal heart.4
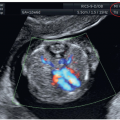
 Figure 3.8: Images of the fetal heart at 11 to 13 weeks of gestation, examined with color Doppler ultrasound. A: Diastolic flow from both right (RA) and left (LA) atrium into the right (RV) and left (LV) ventricle, respectively. B: A normal three-vessel trachea view with aorta (Ao) and pulmonary artery (PA). C: An oblique view showing both left and right ventricular outflow tract in systole with the crossing of Ao and PA. |
Table 3.2 • Image Optimization for Color Doppler Ultrasound in the First Trimester | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


