Fig. 1
A 44-year-old male patient undergoing PET/CT suffering from fever of unknown origin. Contrast-enhanced CT (a), fused PET/CT (b), and PET images (c) are displayed. Increased tracer uptake in the left parotid gland was observed. Warthin’s tumor was confirmed by histopathology
Waldeyer’s ring constitutes of lymphoid tissue located in the naso- and oropharynx including the lingual, the palatinal, and the nasopharyngeal tonsils. Due to the increased tracer uptake of lymphatic cells, tracer uptake can be frequently observed. Still, non-Hodgkin lymphoma and squamous cell carcinomas are frequently found in this location. Although physiological tracer accumulation can be highly variable and range from mild to intense, it is usually symmetrical (Nakamoto et al. 2005; Wong et al. 2007). Therefore, asymmetrical tracer uptake should trigger further investigation, for example, by endoscopy or local inspection (Wong et al. 2007, see Fig. 2).

Fig. 2
64 year old male patient suffering from cancer with unknown primary. Morphological, fused and PET images are displayed for PET/CT (a–c) and PET/MR (d–f). Asymmetrical tracer uptake was noted in the tonsils by PET (right tonsil: SUVmax 10.0; left tonsil: SUVmax 6.2, c and f). The shape of the tonsils was symmetrical and no tumor was detected by contrast enhanced CT (a) or MRI (d). Histopathological sampling during endoscopic evaluation detected a squamous cell carcinoma in the right tonsil
2.1.2 Thyroid
18F-FDG uptake in the thyroid can be highly heterogeneous. Most frequently, a mild to moderate tracer uptake can be observed. In patients with thyroiditis and goiter, however, the overall tracer uptake can be markedly increased (Börner et al. 1998; Yasuda et al. 1998). Special attention has to be paid to focal tracer uptake: In whole-body hybrid imaging examinations, it can be observed with an incidence of up to 4 % in patients without suspected thyroid malignancy. Despite the fact that thyroid adenoma and carcinoma show an increased tracer uptake, malignant cells are detected in up to 36.7 % of all investigated 18F-FDG avid nodules (Choi et al. 2006; Boeckmann et al. 2012; Soelberg et al. 2012).
In histopathological analysis, the most frequently observed malignancy is thyroid carcinoma, as thyroid carcinoma cells are known to overexpress the glucose transport protein GLUT1 and therefore exhibit an increased tracer uptake (Haber et al. 1997). Another, albeit frequently forgotten, reason for focal tracer uptake is metastatic disease of the thyroid gland. Thyroid metastases are typically clinically occult, although they are found in up to 9.5 % of patients dying from a nonthyroid tumor in autopsy studies and can be macroscopically detected in 42 % of these cases. Especially malignant melanoma, breast cancer, renal cancer, head and neck cancer, and colorectal cancer are known to metastasize to the thyroid (Abrams et al. 1950; Shimaoka et al. 1962, see Fig. 3).

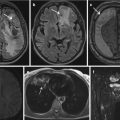
Fig. 3
55 year old male patient who underwent hybrid imaging for staging of recurrent tongue cancer. Morphological, fused and PET images are displayed for PET/CT (a–c) and PET/MR (d–f). The nodule in the left thyroid lobe shows an inhomogeneous appearance and a blurred delineation to the surrounding tissue in CT (a) and MRI (d) as well as a focal FDG-uptake (c and f). The nodule was considered as possibly malignant in both modalities due to the intense tracer accumulation, but neither the morphological information from CT nor from MRI provided additional information. After resection, a thyroid metastasis of a squamous cell carcinoma was histopathologically confirmed
The risk of malignancy is higher in lesions with an increased metabolic activity than in lesions only detected on morphological imaging and demand more thorough investigation. Although some authors proposed cutoff values for the maximum standardized uptake value (SUVmax) to differentiate benign from malignant lesions, more recent publications indicate no significant differences between benign and malignant lesions in SUVmax, even if higher values, in general, might be indicative of a malignant lesion (Choi et al. 2006; Boeckmann et al. 2012). As contrast-enhanced CT does not allow a definite diagnosis of a thyroid nodule, an additional ultrasound examination of the thyroid with fine needle aspiration is recommended by the latest ACR white paper if a focal tracer uptake is detected by 18F-FDG PET and the life expectancy of the patient is not significantly reduced (Hoang et al. 2015).
2.1.3 Larynx
Laryngeal uptake is frequently observed in patients that speak after tracer injection. Symmetrical uptake, for example in the vocal cords, does not pose any diagnostic uncertainty. Palsy of the recurrent laryngeal nerve, caused by prior trauma, thyroid surgery, or local tumor invasion, leads to an increased metabolic activity in the contralateral vocal cord. This asymmetrical tracer uptake can mimic early stage laryngeal cancer or even lymph node metastases in inaccurately fused PET/CT datasets. Here, tracer uptake can be avoided by preventing patients from speaking after tracer injection (Kostakoglu et al. 1996; Purohit et al. 2014).
2.2 Thorax
2.2.1 Lung
Due to the low cellular density of lung parenchyma, overall glucose metabolism in the lungs is low. In combination with CT, tracer uptake due to inflammatory changes can be differentiated from malignant lung lesions in most cases.
In 0.15 % of all PET/CT examinations, intense focal tracer uptake in the lung can be observed that is not related to a pulmonary mass but rather a pulmonary vessel. As these findings are not detectable on follow-up scans, most authors believe that these lesions represent pulmonal microembolism: During radioactive tracer injection via an intravenous line, a small thrombus at the intravenous end of the intravenous line is loaded with a high concentration of 18F-FDG during tracer injection, dissoluted and finally stopped in the pulmonary capillaries (Hany et al. 2003; Chondrogiannis et al. 2015). Even if this finding does not demand any further investigation, the CT and the PET datasets have to be checked for misregistration to exclude malignancy.
2.2.2 Thymus
The thymus is located in the upper ventral mediastinum and harbors an important role in lymphocyte development. While it can be clearly visualized in pediatric patients, the volume of the organ reduces over time and is rarely visible in the adult population. In accordance with organ volume, the 18F-FDG uptake decreases over time (Brink et al. 2001; Nakahara et al. 2001). In patients after chemotherapy or radioactive iodine ablation, however, an enlargement of the thymus and an increased tracer uptake, the so-called thymus rebound, can be sometimes observed and should not be mistaken for metastases or lymphoma (Cohen et al. 1980; Jeon et al. 2014, see Fig. 4).

Fig. 4
48 year old male patient suffering from metastatic rectal cancer undergoing PET/CT for whole-body tumor staging. Morphological CT, fused PET/CT and PET images are displayed before (a–c) and after chemotherapy (d–f). After treatment, a new mass in the anterior mediastinum with a faint tracer uptake can be observed, indicating thymus rebound
2.2.3 Heart
In the regular, nonfasting state, the heart mainly metabolizes carbohydrates, while fasting leads to an increased consumption of fatty acids. As the myocardial layer of the left ventricle is thicker than in the other cavities of the heart, the strongest metabolic activity can be observed here in nonfasting patients. Therefore, the preparation of the patient is highly dependent on the clinical indication. To improve the detection of small tracer avid lesions in oncological patients, it is mandatory that patients fast for at least 4 h prior to 18F-FDG injection. Longer fasting times might be necessary when a lesion is closely related to the myocardium due to the high variability of cardiac glucose consumption (Boellaard et al. 2015).
This high variability can lead to multiple appearances of the heart in 18F-FDG PET, ranging from absent to a diffusely increased 18F-FDG uptake pattern. Furthermore, focal tracer uptake in the papillary muscles as well as regional tracer uptake, most notably in the lateroposterior and in the anterobasal region, is frequent. In patients with coronary artery disease, however, this regional uptake can be altered due to increased glucose consumption of hibernating myocardium (Mäki et al. 1996; Maurer et al. 2011).
In patients with atrial fibrillation, an increased uptake in the atrial wall can be observed that can be mistaken for mediastinal lymph nodes without careful analysis of the fused PET/CT images (Dong et al. 2014, see Fig. 5).

Fig. 5
66 year old male patient undergoing PET/CT for tumor detection with known atrial fibrillation. Contrast enhanced CT (a), fused PET/CT (b) and PET images (c) are displayed. A strong tracer uptake was noted in the left and the right atrium (displayed here) without morphological correlate indicating functional tracer uptake
Rare cases of diffuse tracer uptake are inflammatory diseases such as pericarditis, myocarditis, and epicarditis as well as sarcoidosis, but its relevance in oncological PET imaging has to be evaluated further (James et al. 2011).
Albeit extraordinarily rare, benign as well as malignant cardiac masses can lead to an increased focal tracer accumulation, although a high SUVmax is a strong predictor of malignancy (Nensa et al. 2015). A far more frequent explanation for focal tracer accumulation than a malignant process is lipomatous hypertrophy of the interatrial septum, which is found in up to 2.2 % in CT imaging (Heyer et al. 2003). Albeit not a focal tumor, the increased fatty deposition in the intraatrial septum can show a markedly increase glucose uptake in 18F-FDG PET (Fan et al. 2005; Kuester et al. 2005, see Fig. 6).

Fig. 6
74 year old male patient suffering from metastatic squamous cell carcinoma undergoing PET/CT for whole-body tumor staging. Morphological CT (a), fused PET/CT (b) as well as attenuation corrected (c) and non attenuation corrected (d) PET images are displayed. Increased interatrial fat is observed in morphological CT (a and b) with an increased tracer accumulation that can be observed in the attenuation corrected (c) and non attenuation corrected PET images (d), proving that the increased tracer uptake in the attenuation corrected PET images is not an artifact but indicates a lipomatous hypertrophy of the interatrial septum (LHIAS)
2.2.4 Esophagus and Gastroesophageal Junction
Tracer uptake in the esophagus can be frequently observed, most notably in the gastroesophageal junction. Apart from increased smooth muscle activity, the prevalence of esophagitis seems to be the most common cause (Wu et al. 2014). Due to its focal appearance, it can be easily mistaken for a carcinoma of the esophageal junction. Without a morphological correlate, increased tracer uptake at this location is not a predictor of malignancy (see Fig. 7). The combination of a high SUVmax with a soft tissue mass or focal esophageal wall thickening, however, has to be considered a strong predictor of malignancy (Heusner et al. 2009; Stagg et al. 2014).

Fig. 7
45 year old female patient undergoing PET/CT suffering from an adenomatous cancer with unknown primary after six cycles of chemotherapy. Contrast enhanced CT (a), fused PET/CT (b) and PET images (c) are displayed. Increased functional uptake of the gastroesophageal junction can be observed. A mild reflux esophagitis was discovered during endoscopy
2.3 Abdomen
2.3.1 Stomach and Bowel
Gastrointestinal uptake in the stomach and the bowel is frequently observed in a multitude of different shapes and can be caused by many different reasons. Patchy, segmental, or diffuse tracer enhancement without a morphological correlate originates from 18F-FDG uptake of smooth muscle cells or the mucosa as well as intestinal microorganisms. Especially lymphoid tissue in the cecum can also exhibit a markedly increased tracer uptake (Rosenbaum et al. 2006). Furthermore, inflammatory lesions, for example, in patients with inflammatory bowel disease or patients with gastritis, can show a markedly increased tracer uptake. Special caution is necessary in patients with type 2 diabetes that are treated with metformin, an oral biguanide. Metformin increases glucose consumption in the gastrointestinal tract and leads to a markedly increased, segmental and continuous tracer uptake in the colon and, to a lesser extent, in the small intestine (Bailey 1995; Gontier et al. 2007, see Fig. 8). Although this effect can be reduced by stopping metformin intake 2–3 days prior 18F-FDG PET examinations, no definite recommendations are available concerning 18F-FDG administration and metformin intake (Özülker et al. 2010; Oh et al. 2010; Boellaard et al. 2015).

Fig. 8
63 year old male patient suffering diabetes type 2 who underwent hybrid imaging for whole-body lung cancer staging. Morphological CT (a), fused PET/CT (b) and PET images (c) as well as a PET maximum intensity projection image (d) are displayed. Due to treatment with metformin, an intense tracer uptake can be observed in the colonic wall
Focal tracer uptake in the colon, however, is observed in 1–3 % and associated with a high risk of a malignant or premalignant lesion and demands further colonoscopic evaluation (Kamel et al. 2004; Israel et al. 2005). Still, it has to be kept in mind that although focal tracer uptake in PET/CT has a specificity of 80.2 % for the detection of a colonic pathology, the sensitivity is only 14.8 %. Therefore, the presence of colonic pathologies does not have to coincide with focal tracer uptake (Shim et al. 2012; Keyzer et al. 2015).
2.3.2 Urinary Tract
In the kidneys, a strong tracer uptake of 18F-FDG can be regularly observed as sugars are excreted due to glomerular filtration. In contrast to glucose, however, the radioactive-labeled tracer is not reabsorbed in the tubuli, leading to a markedly increased tracer accumulation in the urinary tract (Rosenbaum et al. 2006). Sometimes, the radioactive urine causes nodal enhancement along the ureter imitating tracer avid lymph nodes on the PET images. In combination with the morphological CT images, the tracer accumulation can be normally clearly attributed to the ureter. Still, the intense tracer accumulation in the bladder caused by the radioactive urine might obscure adjacent lymph nodes.
2.4 Small Pelvis
2.4.1 Female Patients: Uterus and Ovaries
In premenopausal female patients, physiological uptake in the uterus and the ovaries is highly dependent on the menstrual cycle. Especially in the ovulatory phase, a markedly increased 18F-FDG uptake can be observed in the ovaries and the endometrium. Additionally, a strong tracer uptake can be observed in the endometrium during early menstrual flow (see Fig. 9), while no increased tracer uptake is noted in the ovaries at this time. Therefore, it might be advisable to perform 18F-FDG a week before or shortly after menses to exclude physiological tracer uptake if a gynecological malignancy is suspected (Lerman et al. 2004; Nishizawa et al. 2004).

Fig. 9
28 year old female patient suffering from paraganglioma undergoing repeated PET/CT due to increased tracer uptake in disseminated brown adipose tissue. Morphological CT, fused PET/CT and PET images are displayed during the proliferative phase (a–c) and during menstrual flow (d–f). While no tracer uptake in the endometrium can be detected during the proliferative phase, a markedly increased tracer uptake in the endometrium can be observed during mentrual flow
In patients with cervical cancer, an increased endometrial tracer uptake can be observed. However, this is not an indicator of endometrial invasion but is rather induced by local cytokines excreted by the tumor or increased uterine fluid collections caused by a consecutive cervical stenosis. Therefore, PET does not seem to improve the detection of endometrial invasion (Lerman et al. 2004).
In postmenopausal women, physiological tracer uptake in the uterus and the ovaries is rarely observed. In contrast to the glandular tissue in the breast, hormone replacement therapy does not seem to lead to an increased tracer uptake in the ovaries or in the endometrium. Hence, especially increased tracer uptake in the ovaries in postmenopausal women can indicate a malignant process and deserves further investigation (Lerman et al. 2004; Rosenbaum et al. 2006). Despite the high overall sensitivity of 18F-FDG PET for ovarian cancer, only a moderate tracer uptake can be frequently observed in premalignant lesions or early stage cancers. Still, a moderate tracer uptake in the ovaries can also be caused by benign lesions such as endometriomas (Fenchel et al. 2002). Therefore, a close comparison with the morphological images is warranted here.
2.4.2 Male Patients: Prostate and Testes
Incidental tracer uptake in the prostate is detected in about 2 % of all PET/CT studies and is caused by prostate cancer in 17 %. Lesion localization in the peripheral zone and increased patient age seem to be predictors of malignancy, while an association with increased SUVmax is questionable (Bertagna et al. 2015). Still, the positive predictive value for incidental prostate uptake is low as tracer uptake in benign prostatic disease such as prostatitis or benign prostate hyperplasia is common. As the mortality of prostate cancer is low, discretion should be advised when applying invasive techniques to investigate incidental prostatic uptake, especially in oncological patients with a limited life expectancy (Reesink et al. 2015, see Fig. 10).

Fig. 10
A 90-year-old male patient suffering from Merkel cell carcinoma undergoing PET/CT for metastases detection. Contrast-enhanced CT (a), fused PET/CT (b), and PET images (c) are displayed. A strong tracer uptake (SUVmax 10.7) in the prostate indicated prostate cancer, which was confirmed by histopathology
18F-FDG accumulation of the testes is age dependent. While a positive correlation between tracer uptake and patient age can be observed in pediatric patients, glucose metabolism decreases in aging male patients (Kitajima et al. 2007; Goethals et al. 2009). Asymmetrical tracer uptake, however, demands further evaluation as solitary metastases to the testes, or extranodal involvement in lymphoma patients have been reported (Weng and Schöder 2004; Sidhu et al. 2014).
2.5 Bone
In adult patients, hematopoietic bone marrow is replaced by fat. Therefore, the bone marrow normally shows a faint tracer uptake in adults, but in certain cases, this process can be reversed. Due to bone marrow activation after chemotherapy, an increased tracer uptake can be noted in adults. Additionally, intense tracer accumulation in the bone marrow can be observed after recent treatment with granulocyte colony-stimulating factor (Hollinger et al. 1998; Ulaner and Lyall 2013, see Fig. 11).

Fig. 11
A 64-year-old female patient suffering from acute myeloid leukemia and accompanying B-cell non-Hodgkin lymphoma with biopsy-proven bone marrow infiltration undergoing PET/CT after induction chemotherapy. Supportive therapy with granulocyte colony-stimulating factor (G-CSF) was performed until 2 days before the PET/CT examination. Contrast-enhanced CT (a), fused PET/CT (b), and PET images (c) are displayed. A markedly increased tracer uptake in the bone marrow was observed. As no malignant cells were observed in bone marrow biopsy, the tracer uptake in the bone marrow was most likely induced by G-CSF therapy
During the healing process, 18F-FDG tracer uptake can be increased in recent fractures for up to 3 months. Therefore, CT images have to be analyzed carefully to detect acute fractures, postoperative fractures (such as fractures of the rips after thoracotomy for the resection of pulmonary tumors or metastases), and insufficiency fractures, for example, in the sacrum (Zhuang et al. 2003; Fayad et al. 2003). Furthermore, the precise depiction of osteolytic lesions by morphological CT images can be extraordinarily helpful to differentiate benign from malignant fractures.
In elderly patients with osteoarthritis, increased tracer uptake around the acromioclavicular joint, the glenohumeral joint, the hip, or the knee can be found. This uptake is considered to be caused by synovial proliferation in degeneratively changed joints and is rarely associated with symptoms (von Schulthess et al. 2001).
2.6 Inflammatory Lesions and Immunological Responses
Neutrophil granulocytes, monocytes, and macrophages are known to express the glucose transport protein GLUT1 as well as GLUT3 and show an increased hexokinase activity. If these cells are involved in an inflammatory reaction, the markedly increased glucose consumption can be visualized by 18F-FDG PET/CT, leading to a growing number of indications for 18F-FDG PET in inflammatory diseases (Jamar et al. 2013). In oncological 18F-FDG PET imaging, however, it can be difficult to differentiate inflammatory processes from metastatic diseases, especially in patients with suspected lymph node metastases or in lymphoma patients.
Sarcoidosis is a chronic granulomatous disorder. Due to the ongoing inflammatory response, 18F-FDG PET shows a markedly increased tracer accumulation in involved sites and can be therefore used to assess disease extent with a high sensitivity and specificity (Lewis and Salama 1994; Braun et al. 2008). In patients undergoing PET/CT for oncological indications, however, the differentiation between malignant and inflammatory lesions can be challenging. Therefore, it is important not to rely on SUV measurements alone but to analyze the scans under consideration of usual metastatic patterns and suspect sarcoidosis as a possible explanation in the case of an unexpected metastatic spread (Cook et al. 1996, see Fig. 12).

Fig. 12
41 year old male with newly detected mediastinal lympadenopathy. Morphological CT (a), fused PET/CT (b) and PET images (c) as well as a PET maximum intensity projection image (d) are displayed. Mild tracer uptake in mediastinal lymph nodes can be observed, but no primary was detected. Sarcoidosis was confirmed by histopathology after endobronchial ultrasound transbronchial needle aspiration
Infectious diseases are another important pitfall in PET imaging. Especially in immunodeficient patients, opportunistic infectious diseases, such as fungal or mycobacterial infections, can mimic metastatic tumor spread due to disseminated disease (Sharma et al. 2014). As SUV measurements fail to correctly differentiate malignant from infectious lesions, the careful interpretation of the morphological images and ultimately biopsy might be necessary for a definite diagnosis (Rosenbaum et al. 2006).
Another cause for an inflammatory reaction with consecutive tracer uptake is vaccination. After injection, a faint muscular uptake at the vaccination site is frequently observed. Additionally, tracer uptake in the adjacent lymph nodes can be observed up to 1 month after this procedure (Thomassen et al. 2011; Shirone et al. 2012, see Fig. 13). Therefore, it is of utmost importance to identify patients that recently underwent vaccination to reduce the number of false-positive findings. In patients with potential axillary metastases, for example, breast cancer or melanoma patients, it might be advisory to postpone planned vaccination procedures to avoid this potential pitfall.

Fig. 13
Female patient suffering from metastatic breast cancer. Contrast-enhanced CT, fused PET/CT, and PET images of the right upper arm (a–c) and the axillary region (d–f) are displayed. Increased tracer uptake can be noted in the right deltoid muscle (b–c) and in the non-enlarged right axillary lymph nodes (d-f). This patient was vaccinated 14 days prior to 8F-FDG PET/CT. In the follow-up examination 6 months later, no tracer uptake in the right deltoid muscle or the right axillary lymph nodes was observed
2.7 Miscellaneous
2.7.1 Skin and Subcutaneous Fat
Incidental increased tracer uptake in the skin is most frequently caused by inflammation. Especially focal inflammation, e.g., in infected atheroma or acne, can show an increased tracer uptake due to the increased presence of lymphatic cells. Apart from bacterial infections, viral infections such as an active herpes zoster infection can lead to an increased cutaneous tracer uptake that might even involve the associated lymph nodes (Wadih et al. 2015).
A rare inflammatory disease is hidradenitis suppurativa involving the hair follicles that can be predominantly found in the inguinal, perianal, and axillary region (see Fig. 14). Here, an intense tracer accumulation can be discovered involving the cutaneous tissue and the subcutaneous fat and can lead to fistulas and even osteomyelitis as well as malignant transformation (Simpson et al. 2011; Poh and Wong 2014). In most of the cases, diagnostic security can be increased by mere inspection which should therefore not be omitted.

Fig. 14
51 year old male patient suffering from malignant melanoma who underwent hybrid imaging for whole-body staging. Morphological CT (a), fused PET/CT (b) and PET images (c) as well as a PET maximum intensity projection image (d) are displayed. Intense tracer uptake in the left axillary region with cutaneous thickening was suspicious of a second malignant melanoma. Local inspection showed a local inflammation in a patient with known hidradenitis suppurativa in the axillary region
2.7.2 Brown Adipose Tissue
Apart from the predominant white adipose tissue, brown adipose tissue can be found especially in young female patients and children. In contrast to white adipose tissue, which its primary ability is fat deposition, brown adipose tissue can generate warmth by the metabolization of triglycerides and sugars, especially in cold environments. If these patients are not kept warm during the uptake phase and the PET scan, symmetrical tracer uptake can be observed most frequently in the head and neck area but also in the mediastinum and the perivertebral fatty tissue. Although brown adipose tissue can be correctly identified on fused PET/CT images by the pattern of distribution and identification of fat as morphological correlate of focal tracer uptake, small tracer avid lesions that are also situated in the fatty tissue, such as lymph node metastases, can be obscured. Therefore, it can be advisory to prepare patients with known high activity of brown adipose tissue by keeping the patients warm after 18F-FDG injection (Boellaard et al. 2015). Furthermore, pharmacological means to decrease the glucose uptake in brown adipose tissue have been explored, for example, by administering propanolol or diazepam prior to tracer injection (Söderlund et al. 2007; Rakheja et al. 2011, see Fig. 15).

Fig. 15
28 year old female patient suffering from paraganglioma undergoing repeated PET/CT due to increased tracer uptake in disseminated brown adipose tissue. PET maximum intensity projection images are displayed. In the initial scan, a markedly increased tracer uptake can be observed in brown adipose tissue in the cervical and the mediastinal area (a). The second scan was performed after propanolol administration. Furthermore, the patient was kept warm during the tracer uptake phase, leading to a markedly reduced tracer accumulation in the brown adipose tissue (b)
A rare variant is hibernoma, a benign tumor consisting of brown adipose tissue (Furlong et al. 2001, see Fig. 16). While the tumor mimics a lipoma in morphological imaging, it exhibits an extraordinary high tracer uptake in PET imaging. Although hibernomas neither do show signs of tumor invasion of the surrounding tissues nor solid components, it still cannot be differentiated from highly differentiated liposarcoma in morphological imaging. A possible tool of differentiation is a repeated PET imaging as strong SUV fluctuations of hibernomas have been observed in small cohorts (Smith et al. 2008). Still, histopathological correlation is necessary for a definite diagnosis.

Fig. 16
A 72-year-old female patient suffering from a motoneuron disease of unknown origin undergoing PET/CT for tumor detection. Contrast-enhanced CT (a), fused PET/CT (b), and PET images (c) are displayed. A fatty lesion without local tumor invasion was detected in the left upper thigh with an increased tracer uptake without septae. In the histopathological examination of the resection specimen after tumor resection, the diagnosis of a hibernoma was confirmed
2.7.3 Breast
Tracer uptake in the breast is observed in the glandular mammary tissue and can therefore be mainly observed in premenopausal women and postmenopausal women undergoing hormone replacement therapy. Intense tracer uptake of both breasts is frequently found in lactating women (see Fig. 17) but can also be asymmetrical if the child is predominantly fed from one side (Abhyankar et al. 2012). Therefore, especially small lesions can be obscured by the increased glandular uptake and can be difficult to detect in the PET dataset. Focal 18F-FDG uptake in the breast, however, is a strong predictor of malignancy and demands further investigation (Bertagna et al. 2015).

 Findings – Ethical Aspects
of Incidental Findings on Multimodal Imaging in UK Biobank
Findings and Their Handling in the Swedish CArdioPulmonary bioImage Study (SCAPIS)
Findings – Ethical Aspects
of Incidental Findings on Multimodal Imaging in UK Biobank
Findings and Their Handling in the Swedish CArdioPulmonary bioImage Study (SCAPIS)
 of Incidental Findings in the German National Cohort
of Incidental Findings in the German National Cohort
 of Incidental Findings in the Study of Health in Pomerania
of Incidental Findings in the Study of Health in Pomerania
 Findings in a Population Based Study Using Cardiac CT: Experience from the Multi-Ethnic Study of Atherosclerosis (MESA)
Findings in a Population Based Study Using Cardiac CT: Experience from the Multi-Ethnic Study of Atherosclerosis (MESA)




Related posts:
Findings – Ethical Aspects
of Incidental Findings on Multimodal Imaging in UK Biobank
Findings and Their Handling in the Swedish CArdioPulmonary bioImage Study (SCAPIS)
of Incidental Findings in the German National Cohort
of Incidental Findings in the Study of Health in Pomerania
Findings in a Population Based Study Using Cardiac CT: Experience from the Multi-Ethnic Study of Atherosclerosis (MESA)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
