Fig. 20.1
Transverse ultrasound image of the right lobe demonstrates a thin-walled anechoic structure with posterior acoustic enhancement in the thyroid gland. This is a simple benign cyst

Fig. 20.2
Transverse ultrasound image of the right lobe of the thyroid demonstrating a mixed solid and cystic nodule. Targeted FNA of the solid portion of the lesion revealed papillary thyroid carcinoma
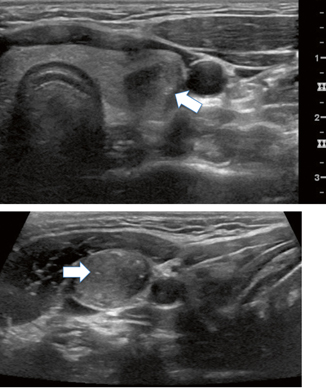
Fig. 20.3
a Transverse thyroid ultrasound image reveals microcalcifications (arrow) within a solid nodule in the left lobe of the thyroid. Fine needle aspiration of the lesion was significant for papillary thyroid carcinoma. b Transverse image of lymph node in the right neck adjacent to the carotid artery in the same patient. Note the similar sonographic appearance to the primary thyroid lesion (arrow)
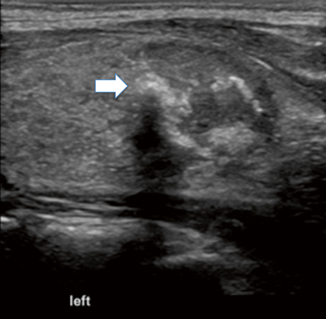
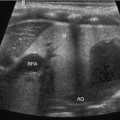
Fig. 20.4
Coarse calcifications within a right thyroid nodule. Note the posterior shadowing from the calcifications (arrow). FNA revealed papillary cancer
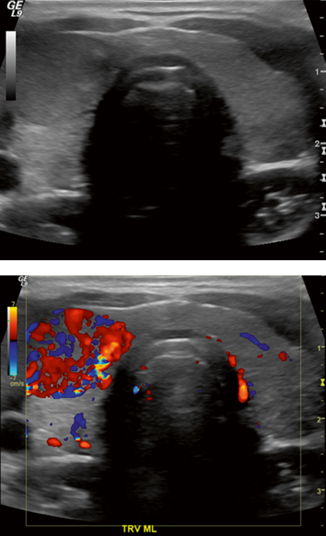
Fig. 20.5
a Transverse ultrasound images of the thyroid in a 10-year-old female. A dominant nodule path proven to be papillary thyroid carcinoma is noted within the right lobe of the thyroid. b Color Doppler demonstrates hypervascularity of the lesion
Based on the SRU consensus statement, fine needle aspiration (FNA) is suggested for a thyroid nodule of 1.0 cm or larger if microcalfcifications are present, 1.5 cm or larger if the nodule is solid with coarse calcifications, 2 cm with mixed solid and cystic components, or nodules that have substantial growth over an interval period [6]. As reflected in the SRU guidelines, ultrasound characteristics are more important than size when determining whether a nodule should be sampled.
The cytopathology result of the FNA determines whether observation, repeat FNA, or surgery should be performed. With respect to the cytopathology result, the Bethesda Classification System for Reporting Thyroid Cytopathology allows for standardization which in turn dictates management [7]. Every FNA report groups the cytopathology into six distinct categories. Each category has an associated risk for malignancy and a recommended management scheme (Table 20.1).
Table 20.1
The Bethesda classification system for thyroid malignancy
Classification | Risk of malignancy (%) | Management |
|---|---|---|
Nondiagnostic | 1–4 | Repeat FNA |
Benign | <5 | Follow up ultrasound in 6–18 months |
Follicular lesion of uncertain significance | 5–15 | Follow up ultrasound +/− repeat FNA in 3–6 months |
Follicular neoplasm, Hürthle cell neoplasm | 20–30 | Surgical lobectomy |
Suspicious for papillary thyroid cancer | 60–75 | Thyroid lobectomy/total thyroidectomy |
Papillary thyroid cancer | 98 | Total thyroidectomy |
FNA in children presents a unique challenge as opposed to adults. While most adults can lie still for an FNA , children may require local anesthesia, intravenous conscious sedation, or even general anesthesia. Anesthesia does carry inherent risks and every case should undergo an appropriate risk/benefit analysis. However, it is best to err on the side of increased patient comfort and hence decreased patient motion as adjacent structures can be inadvertently damaged even with a small-gauge needle.
Some practitioners perform FNA of thyroid without ultrasound. Although ultrasound guidance may add slightly to the cost and length of the procedure, it is felt to provide more accurate diagnostic information. This is particularly true when nodules cannot be palpated, when there is some alteration in anatomy, and when a specific thyroid nodule needs to be sampled in the setting of multiple nodules. Additionally, ultrasound allows for targeting of the solid components of a lesion that has mixed solid and cystic characteristics and allows for the visualization of larger vasculature that should be avoided.
Pre-procedural Management
The most important aspect of pre-procedural management is confirming that there is a documented indication for the biopsy. All prior imaging studies should be reviewed. Most practitioners agree that anticoagulants, including antiplatelet agents, should be held for 4–7 days prior to the FNA procedure. In some instances, antiplatelet agents may be difficult to hold. Thyroid lesions can still be safely biopsied in this clinical setting as long as the procedure is meticulously performed. Informed consent with documentation of the risks of the procedure should be obtained from the patient or legal guardian. It is also prudent to discuss each case individually with the anesthesia provider to determine whether local anesthetic alone, intravenous sedation, or general endotracheal anesthesia will be required. If the institution has the capability, having an on-site cytopathologist during the procedure can eliminate unnecessary needle passes through the thyroid lesion and limit the amount of nondiagnostic biopsies.
Technique
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


