Fig. 1
Removal of large fibroids
2.1.2 Desire Fertility with Short Time Window
The combination of UAE and myomectomy for myoma is indicated for women who desire uterine preservation and fertility within a short time window. UAE can aid in treatment of myoma with subsequent myomectomy by ensuring no potential for regrowth given successful embolization. Myomectomy alone may not completely ensure uterine preservation because of the possibility of fibroid recurrence and subsequent myomectomy (Hanafi 2005) or surgical conversion from myomectomy to hysterectomy (Subramanian et al. 2001). UAE alone is not a contraindication for fertility. Pregnancy following UAE is not uncommon (McLucas 2013); however some complications of UAE may affect ability to achieve a viable pregnancy (Mara et al. 2012). Thus myomectomy combined with embolization may increase the likelihood of subsequent pregnancies (Nabeshima et al. 2003).
Our guidelines for UAE as a stand-alone procedure for women desiring fertility are as follows. The uterus should be less than the size of a 10-week gestation. The position of the myomas should be intramural to subserosal. The largest myoma should be less than 8 cm. Our percentage of patients who conceived without combination procedures was 48 % in women under 40 who stated a desire for fertility (McLucas 2013). We, however, are sensitive to the woman in her late 30s desiring fertility. We recommend that patients wait 6 months after UAE before conception (McLucas 2013). If patients feel that such a wait is too long, and with the possibility of additional wait time if the UAE is not successful, we will offer the patient the combination procedure. Patients need to be told that the combination procedure in this circumstance is optional.
UAE prior to myomectomy is an appropriate approach for treatment of fibroids in women who wish to achieve pregnancy shortly following treatment (Nabeshima et al. 2003). Generally women can begin to try to achieve pregnancy after 6 months after having UAE and myomectomy, the same amount of time for UAE alone. Concerning future pregnancies, UAE may be beneficial for women in whom extensive pelvic adhesions following myomectomy may result in a high possibility for hysterectomy. Such patients with extensive adhesions may require in vitro fertilization, and should be told such prior to any other procedure.
2.1.3 Pedunculated Submucous or Subserous Myomas
Some authors have said that pedunculated submucous or subserous myomas are often considered a contraindication for UAE because of potential risks and complications, including ischaemic necrosis and separation from the uterus due to torsion at the stalk of the myoma (Levy 2008; Al-Fozan and Tulandi 2002). However in these cases, the only option may be a complicated myomectomy or hysterectomy. Women may opt for UAE if they do not want to undergo invasive surgery or wish to preserve their uterus. UAE has been suggested to be a viable and safe form of treatment for pedunculated subserous myomas with a relatively small stalk diameter and these major complications may be rare (Katsumori et al. 2005). UAE may be useful prior to myomectomy for these types of fibroids because it facilitates easier removal of the fibroid. There is no need for gonadotropin-releasing-hormone agonists prior to myomectomy (Paxton et al. 2006). The outcome is better for patients with submucous and subserous myomas when undergoing myomectomy after uterine artery embolization as a pre-treatment (Butori et al. 2011).
First, hysteroscopic resection will have relatively decreased blood loss after embolization (Wamsteker et al. 1993; Walker and Barton-Smith 2006). The surgeon will have less worry about fluid absorption following embolization (Al-Mahrizi and Tulandi 2007). Thus, the hysteroscopic removal of pedunculated submucous myoma will be facilitated by prior embolization as well as allowing the surgeon to attack a larger myoma (Walker and Barton-Smith 2006). Pre-treatment with UAE decreases blood flow to a pedunculated subserous myoma, again allowing the surgeon the opportunity to remove a larger myoma that might be possible without prior embolization (Butori et al. 2011). A combination of UAE and myomectomy may be the optimum choice in these instances because it maximizes the benefits of both procedures for women choosing invasive but conservative treatment options.
Furthermore, a combination of UAE with either hysteroscopic or laparoscopic myomectomy will greatly diminish the incidence of necrosis following embolization (Al-Fozan and Tulandi 2002). The first reported death due to uterine sepsis was reported to have been found with a submucosal myoma (Vashisht et al. 1999) (Fig. 2).

Fig. 2
Prolapsing submucous myoma
2.2 Benefits of UAE Prior
2.2.1 Decrease Blood Loss
UAE is beneficial prior to myomectomy in cases where periprocedural blood loss may be substantial (Ngeh et al. 2004). To reduce the possibility of excessive blood loss when removing fibroids, UAE has been successfully used prior to myomectomy (Butori et al. 2011; Serradilla et al. 2011). The advantages of using UAE for minimizing blood loss allow for more endoscopic approaches to complicated myomectomies. Surgery for multiple myomas may allow for tumor size reduction prior to surgery, which may decrease the possibility of conversion to hysterectomy. This is because tumor infarction occurs immediately following UAE. This combination procedure may also decrease hospital stay, as many potential postoperative complications may be avoided such as pyrexia due to hematoma (Dumousset et al. 2008). The technical removal of myomas may be easier with UAE prior. This includes removal of significantly reduced fibroid volume and ease of uterine suturing (Tixier et al. 2008).
Management of blood loss may also allow for laparoscopic removal of larger fibroids. To date, the largest fibroid reported to be removed by this method was larger than 20 cm (Madhuri et al. 2010). Generally, laparoscopic myomectomies are limited by myoma size because of the limited amount of space to manipulate the laparoscopic instruments. Laparoscopic myomectomy is the preferred method of myomectomy due to shorter hospital stay, less postoperative pain, and reduced risk of adhesions. Thus, by reducing potential blood loss through UAE larger myomas may be removed through this preferred method.
2.2.2 No Fibroid Recurrence
Although myomectomies seek to remove current fibroids and diffuse symptoms, fibroid recurrence remains a possibility. UAE prior to myomectomy prevents myoma regrowth because the tumors have been devascularized. Combining two procedures during one hospital admission has many advantages including those economically and logistically related. The recurrence rate following myomectomy has been reported to be as high as 75 % in some studies (Hanafi 2005). Because the surgery occurs immediately following the procedure, no time exists for collateral vessel formation.
2.2.3 Candidates
Some patients may benefit from myomectomy scheduled after UAE. This includes patients with large uterine fibroids with a high risk of excessive menorrhagia who wish to preserve their uterus or who do not wish to receive a blood transfusion. Young patients tend to fall in this category because they are farther from reaching menopause, in which fibroid growth generally ceases because the ovaries stop producing estrogen.
2.2.3.1 Young Patients with High Risk of Recurrence
Studies have shown that younger patients who undergo myomectomy are at higher risk of fibroid recurrence and subsequent surgery. Reed et al. found that 5 years after myomectomy, the age-specific cumulative incidence of a subsequent uterine surgery was greatest in women aged 30–34 years (38 %), which increased to 44 % at 7-year follow-up. The total incidence of repeat surgery is 20.2 %, which included repeat myomectomy and hysterectomy (Reed et al. 2006). This increased risk may also be related to whether the patient has completed childbearing at the time of consideration of a second surgery. The risk of recurrence may be diminished if the patient becomes pregnant following the initial procedure (Candiani et al. 1991).
2.2.3.2 Patients Ready for Childbearing After 6 months
Myomectomy is suggested as the optimal fibroid treatment for women desiring future fertility (van der Kooij et al. 2012). Pregnancy is possible following myomectomy, but increased risk of uterine rupture due to adhesions and caesarian section may complicate childbirth (Goldberg and Pereira 2006; Lumsden 2002). UAE prior to myomectomy reduces the risk of adhesion formation. Adhesion formation is a known complication of abdominal or laparoscopic myomectomy (Butori et al. 2011). Although some adhesion formation have been reported following embolization, the incidence of this complication is unknown (Agdi et al. 2008). Furthermore, UAE and myomectomy in combination allows for removal of fibroids that may complicate pregnancy without the possibility of fibroid regrowth. Women may begin to try to conceive after 6 months of this combination procedure during the “golden period” because that is when myomas are less likely to recur (Candiani et al. 1991).
2.3 Surgical Technique
Myomectomy after UAE allows both the surgeon and the patient benefits compared to stand-alone myomectomy. We will address differences in laparotomy, laparoscopy, and hysteroscopy for myomectomy. Abdominal myomectomy is our preferred technique for multiple intramural myomata. We use this as the technique for large uteri as well. If the myomectomy is performed within 2 weeks of the UAE procedure, surgeons will be pleased by the almost bloodless field encountered. We have not had to convert any of our myomectomy patients to hysterectomy because of blood loss after embolization.
After 3 months, the amount of blood loss will increase, but not to the level of patients who have not undergone UAE. Myomectomy performed after 3 months is most commonly performed for a necrotic myoma. This condition is associated with malodorous discharge, and liquifications (Fig. 3). Cultures of the material within the myoma should be obtained, both aerobic and anaerobic. During the myomectomy, margins of the myoma and healthy myometrium may be blurred. Care should be taken to remove as much necrotic material as possible from the margins. We use manual pressure with lap sponges and gauze pads to aid in this process. A point of advise: the surrounding myometrium is invariably healthy, once the necrotic myoma is removed. We have only performed one hysterectomy (McLucas et al. 2001) on a patient post embolization with symptoms of necrosis. This was at the request of the patient.
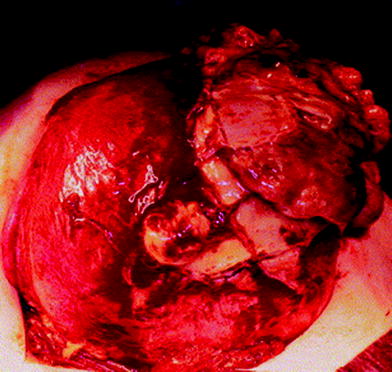
Fig. 3
Necrotic myoma
During the post-operative myomectomy period when the procedure is performed for a necrotic myoma, we routinely continue broad spectrum antibiotic coverage for 7–10 days gram negative and anaerobic bacteria. This generally includes combination of antibiotics such as gentamycin and clindamycin (Spies et al. 2002). For patients with a penicillin allergy, vancomyocin is used (Weed 2003). No study has shown that the use of prophylactic antibiotics prevents infection after UAE, however it is suggested that prophylactic antibiotics reduce the risk of sepsis (Walker et al. 1999). Our patients often experience some febrile morbidity, and leukocytosis from bacteria at the margins of myomata. In spite of this, we have not had to perform a hysterectomy for post-operative infection. We counsel our patients prior to surgery of the likelihood of fever, and perhaps an extra day or two for antibiotic therapy.
2.3.1 Laparoscopic Myomectomy
If performed within the first 2 weeks post-operative after UAE, the surgeon will again benefit from a bloodless field. We offer patients with large pedunculated subserous myomata the option of a combination UAE followed by laparoscopic myomectomy for symptom relief. Patients are told about the risks of a second procedure performed under general anesthesia. This is balanced by reports of pedunculated subserous myomata becoming necrotic post UAE (Katsumori et al. 2005). Also discussed is the relief of pain immediately after myomectomy, as opposed to waiting the 6 months for shrinkage after UAE. If on pelvic examination prior to UAE, the patient complains of pain when examining the area of pedunculated myoma, we will take this into consideration as well to offer patients a combination laparoscopic myomectomy and embolization (Dumousset et al. 2008




Related posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
