Foreign Body—Ultrasound
Kelly L. Hastings
Daniel B. Nissman
CLINICAL HISTORY
20-year-old male with hand injury while hiking.
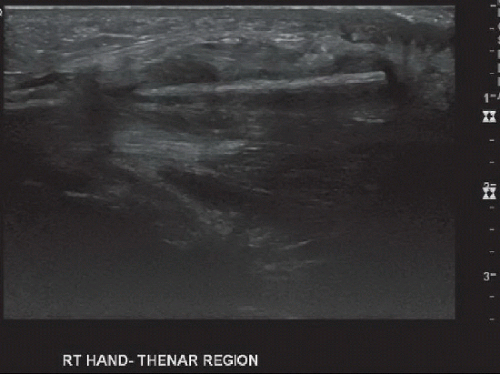 FIGURE 86A |
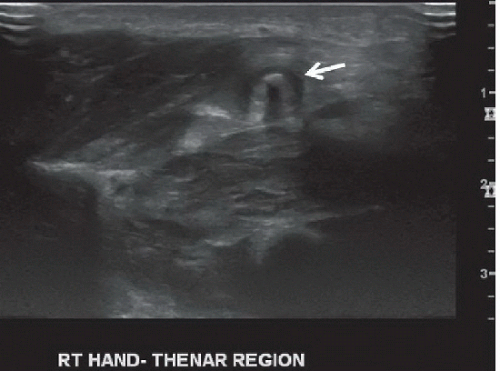 FIGURE 86B |
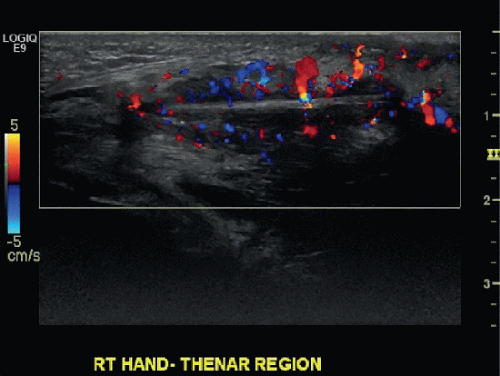 FIGURE 86C |
FINDINGS
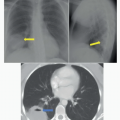
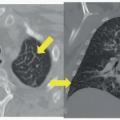
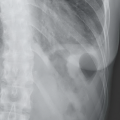
Long (Fig. 86A) and short (Fig. 86B) axis sonographic images of the thenar eminence of the right hand demonstrate a 2.8-cm long, linear, echogenic structure (arrow on short-axis image) surrounded by a halo of hypoechogenicity located nearly 1 cm deep to the skin surface. There is posterior acoustic shadowing with comet-like hyperechogenicity projecting deep to the structure at the edges. Doppler evaluation (Fig. 86C) reveals marked surrounding vascularity.
DIFFERENTIAL DIAGNOSIS
Foreign body, soft tissue calcification, or soft tissue tumor.
DIAGNOSIS
Foreign body (wood splinter) with surrounding edema and inflammation.
DISCUSSION
Retained foreign bodies can result from any penetrating trauma, commonly motor vehicle accidents or industrial accidents. Metal, wood, and glass foreign bodies are most common. Foreign bodies are easily missed; 38% of foreign bodies are missed on initial evaluation.1 Early detection is important, as retained foreign bodies act as a nidus for infection or granulomatous reactions.
Radiographs will demonstrate foreign bodies only if the difference in densities between the foreign body and surrounding soft tissues is sufficiently high to make detection possible. Although glass is nearly universally detectable radiographically in the extremities,2 for wood foreign bodies the difference in density is often too small to be appreciated on radiographs. Ultrasonography is the preferred imaging modality for suspected superficial foreign bodies because of its ease of use, low cost, and lack of ionizing radiation. Ultrasonography can also be used to facilitate foreign body removal.
A high-frequency ultrasound transducer, which provides excellent near-field resolution, is preferred because most retained foreign bodies are located in the superficial soft tissues. Modern transducers have excellent near-field imaging characteristics; a standoff pad is usually not required, but could be considered especially if dermal involvement is suspected. The sonographic appearance of foreign bodies depends on the acoustic properties of the foreign material; however, all foreign bodies so far studied appear echogenic.3 Posterior acoustic shadowing depends on the surface of the foreign body with flat surfaces producing dirty shadows and reverberation artifact because of multiple backscattered echoes detected by the transducer, while irregular surfaces produce clean shadowing because of ultrasound waves being scattered at different angle causing loss of signal to the transducer.3 Hyperechoic or hypoechoic streaks may be
observed at the edges of a retained foreign body. Edema surrounding a foreign body can produce a hypoechoic halo. Doppler interrogation will reveal adjacent hyperemia in proportion to the degree of associated inflammation. A recent meta-analysis of 17 studies showed a pooled sensitivity of 72% and specificity of 92% for the sonographic detection of any soft tissue foreign body and a pooled sensitivity of 96.7% and specificity of 84.2% in a subgroup analysis for the detection of radiolucent foreign bodies including wood.4 Cadaver studies have demonstrated a sensitivity of 87% and specificity of 97% for the sonographic detection of 2.5 mm long wooden foreign bodies with increased sensitivity with increased size.5 Potential false-positive findings include gas, soft tissue calcifications including bone fragments, and granulomas.
observed at the edges of a retained foreign body. Edema surrounding a foreign body can produce a hypoechoic halo. Doppler interrogation will reveal adjacent hyperemia in proportion to the degree of associated inflammation. A recent meta-analysis of 17 studies showed a pooled sensitivity of 72% and specificity of 92% for the sonographic detection of any soft tissue foreign body and a pooled sensitivity of 96.7% and specificity of 84.2% in a subgroup analysis for the detection of radiolucent foreign bodies including wood.4 Cadaver studies have demonstrated a sensitivity of 87% and specificity of 97% for the sonographic detection of 2.5 mm long wooden foreign bodies with increased sensitivity with increased size.5 Potential false-positive findings include gas, soft tissue calcifications including bone fragments, and granulomas.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


