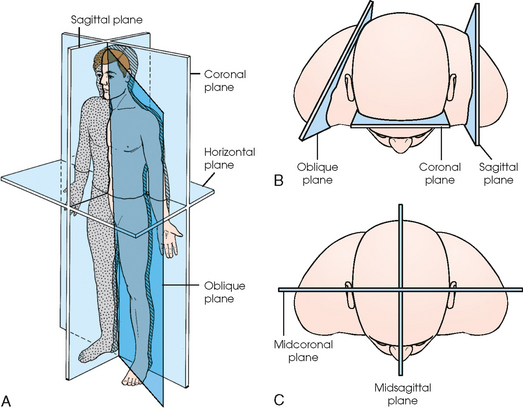
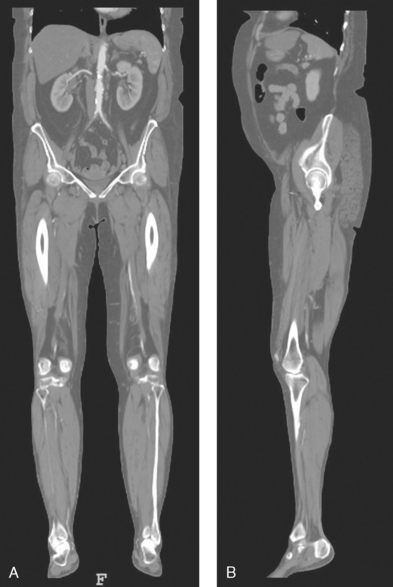
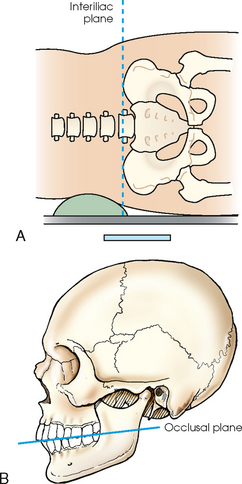
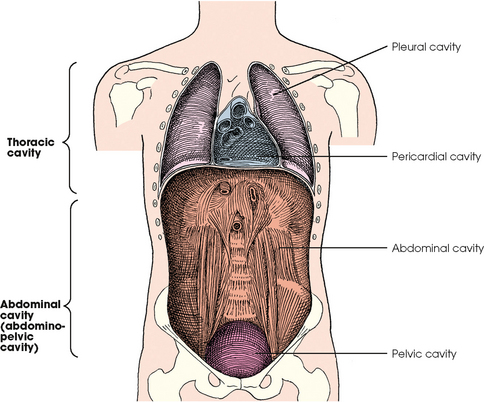
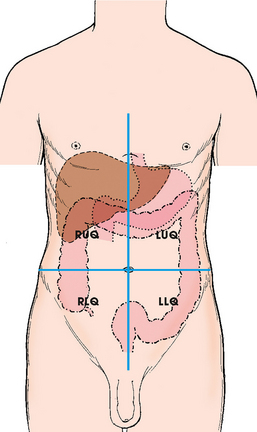
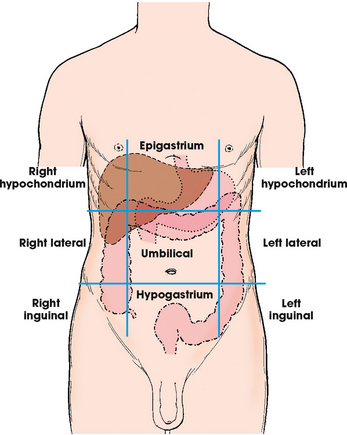
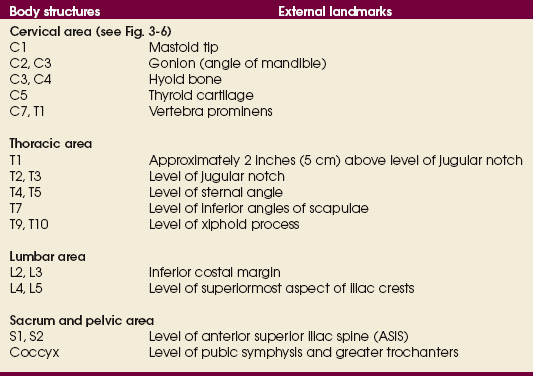
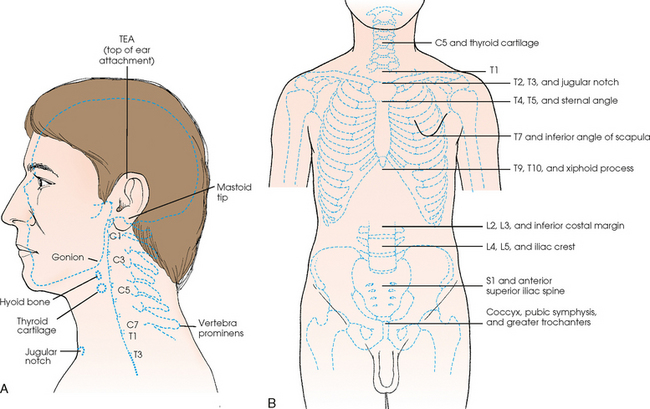
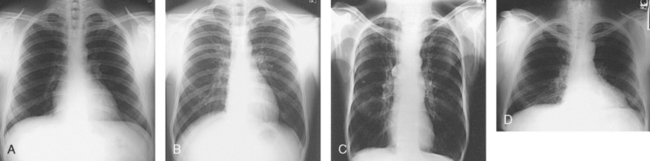
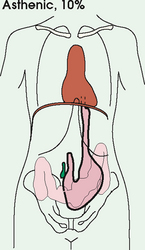
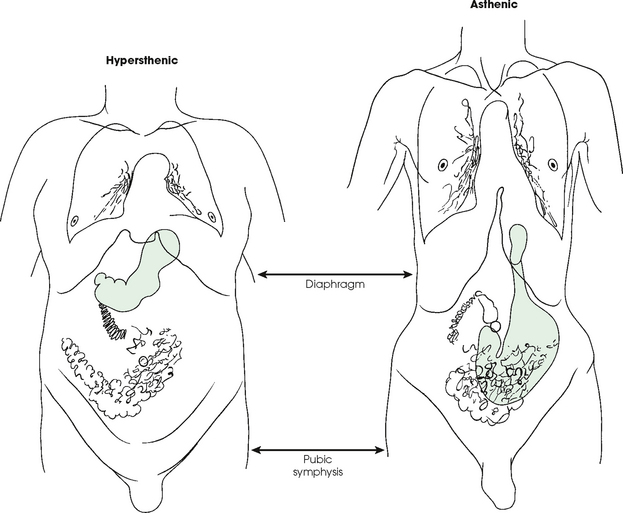
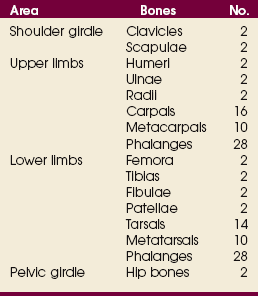
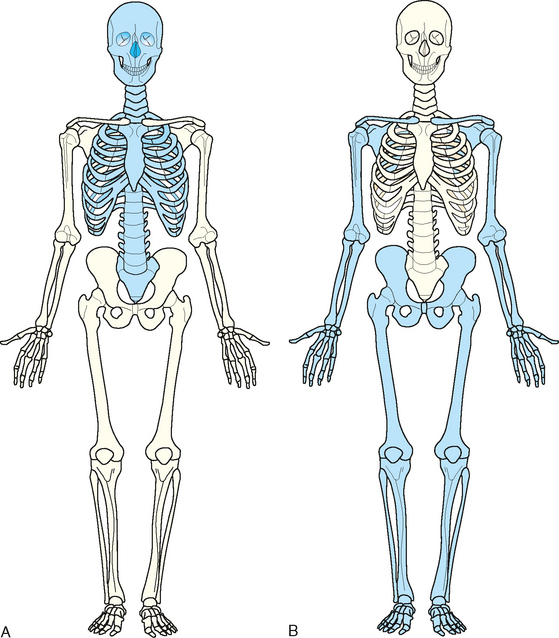
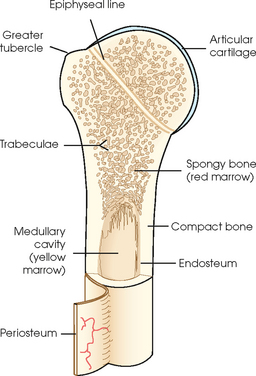
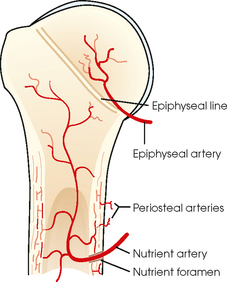
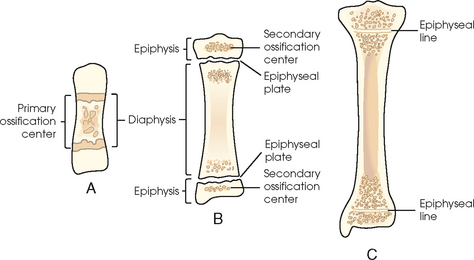
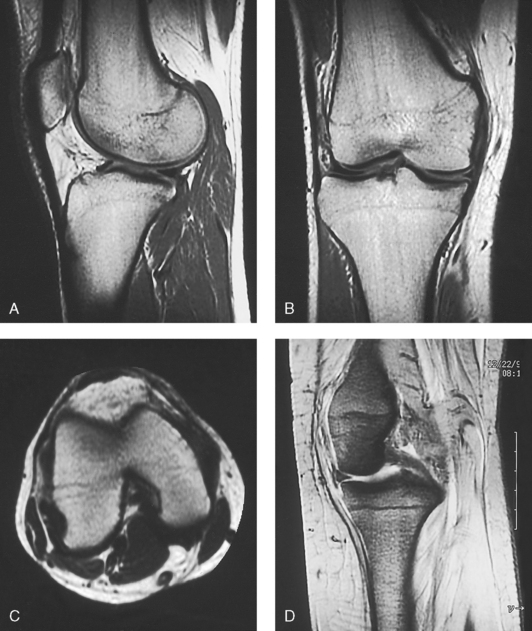
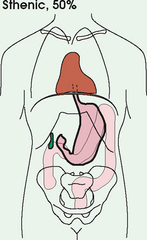
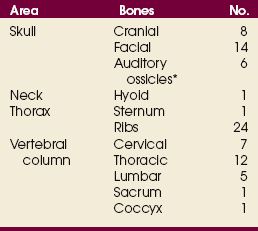
3 The full dimension of the human body as viewed in the anatomic position (see Chapter 1) can be effectively subdivided through the use of imaginary body planes. These planes slice through the body at designated levels from all directions. The following four fundamental body planes referred to regularly in radiography are illustrated in Fig. 3-1, A: A sagittal plane divides the entire body or a body part into right and left segments. The plane passes vertically through the body from front to back (see Fig. 3-1, A and B). The midsagittal plane is a specific sagittal plane that passes through the midline of the body and divides it into equal right and left halves (Fig. 3-1, C). A coronal plane divides the entire body or a body part into anterior and posterior segments. The plane passes through the body vertically from one side to the other (see Fig. 3-1, A and B). The midcoronal plane is a specific coronal plane that passes through the midline of the body, dividing it into equal anterior and posterior halves (see Fig. 3-1, C). This plane is sometimes referred to as the midaxillary plane. A horizontal plane passes crosswise through the body or a body part at right angles to the longitudinal axis. It is positioned at a right angle to the sagittal and coronal planes. This plane divides the body into superior and inferior portions. Often it is referred to as a transverse, axial, or cross-sectional plane (see Fig. 3-1, A). An oblique plane can pass through a body part at any angle among the three previously described planes (see Fig. 3-1, A and B). Planes are used in radiographic positioning to center a body part to the image receptor (IR) or central ray and to ensure that the body part is properly oriented and aligned with the IR. The midsagittal plane may be centered and perpendicular to the IR with the long axis of the IR parallel to the same plane. Planes can also be used to guide projections of the central ray. The central ray for an anteroposterior (AP) projection passes through the body part parallel to the sagittal plane and perpendicular to the coronal plane. Quality imaging requires attention to all relationships among body planes, the IR, and the central ray. Body planes are used in computed tomography (CT), magnetic resonance imaging (MRI), and ultrasound (US) to identify the orientation of anatomic cuts or slices shown in the procedure (Fig. 3-2). Imaging in several planes is often used to show large sections of anatomy (Fig. 3-3). Fig. 3-2 MRI of the knee in four planes. A, Sagittal. B, Coronal. C, Horizontal. D, Oblique, 45 degrees. The interiliac plane transects the pelvis at the top of the iliac crests at the level of the fourth lumbar spinous process (Fig. 3-4, A). It is used in positioning the lumbar spine, sacrum, and coccyx. The two great cavities of the torso are the thoracic and abdominal cavities (Fig. 3-5). The thoracic cavity is subdivided into a pericardial segment and two pleural portions. Although the abdominal cavity has no intervening partition, the lower portion is called the pelvic cavity. Some anatomists combine the abdominal and pelvic cavities and refer to them as the abdominopelvic cavity. The principal structures located in the cavities are listed on the following page. The abdomen is often divided into four clinical divisions called quadrants (Fig. 3-6). The midsagittal plane and a horizontal plane intersect at the umbilicus and create the boundaries. The quadrants are named as follows: Many commonly used landmarks are listed in Table 3-1 and diagrammed in Fig. 3-8. These landmarks are accepted averages for most patients and should be used only as guidelines. Variations in anatomic build or pathologic conditions may warrant positioning compensation on an individual basis. The ability to compensate is gained through experience. Common variations in the shape of the human body are termed the body habitus. 1 determined the primary classifications of body habitus based on his study of 1000 patients. The specific type of body habitus is important in radiography because it determines the size, shape, and position of the organs of the thoracic and abdominal cavities. Body habitus directly affects the location of the following: An organ such as the gallbladder may vary in position by 8 inches, depending on the body habitus. The stomach may be positioned horizontally, high, and in the center of the abdomen for one type of habitus and positioned vertically, low, and to the side of the midline in another type. Fig. 3-9 shows an example of the placement, shape, and size of the lungs, heart, and diaphragm in patients with four different body habitus types. Box 3-1 describes specific characteristics of the four types of body habitus and outlines their general shapes and variations. The four major types of body habitus and their approximate frequency in the population are identified as follows: BOX 3-1 Four types of body habitus: prevalence, organ placement, and characteristics Heart: Nearly vertical and at midline Lungs: Long, apices above clavicles, may be broader above base Stomach: Low and medial, in the pelvis when standing Heart: Axis nearly transverse Lungs: Short, apices at or near clavicles Stomach: High, transverse, and in the middle Colon: Around periphery of abdomen Radiographers must also become familiar with the two extreme habitus types: asthenic and hypersthenic. In these two small groups (15% of the population), the placement and size of the organs significantly affect positioning and the selection of exposure factors. Consequently, radiography of these patients can be challenging. Experience and professional judgment enable the radiographer to determine the correct body habitus and to judge the specific location of the organs. Body habitus is not an indication of disease or other abnormality, and it is not determined by the body fat or physical condition of the patient. Habitus is simply a classification of the four general shapes of the trunk of the human body. When positioning patients, the radiographer should be conscious that habitus is not associated with height or weight. Four patients of equal height could have four different trunk shapes (Fig. 3-10). • Mechanical basis for movement • Protection of internal organs • Storage for calcium, phosphorus, and other salts The 206 bones of the body are divided into two main groups: The axial skeleton supports and protects the head and trunk with 80 bones (Table 3-2). The appendicular skeleton allows the body to move in various positions and from place to place with its 126 bones (Table 3-3). Fig. 3-11 identifies these two skeletal areas. TABLE 3-2 *Auditory ossicles are small bones in the ears. They are not considered ofofficial bones of the axial skeleton but are placed here for convenience. The general features of most bones are shown in Fig. 3-12. All bones are composed of a strong, dense outer layer called the compact bone and an inner portion of less dense spongy bone. The hard outer compact bone protects the bone and gives it strength for supporting the body. The softer spongy bone contains a spiculated network of interconnecting spaces called the trabeculae (Fig. 3-13). The trabeculae are filled with red and yellow marrow. Red marrow produces red and white blood cells, and yellow marrow stores adipose (fat) cells. Long bones have a central cavity called the medullary cavity, which contains trabeculae filled with yellow marrow. In long bones, the red marrow is concentrated at the ends of the bone and not in the medullary cavity. Bones are live organs and must receive a blood supply for nourishment or they die. Bones also contain a supply of nerves. Blood vessels and nerves enter and exit the bone at the same point, through openings called the foramina. Near the center of all long bones is an opening in the periosteum called the nutrient foramen. The nutrient artery of the bone passes into this opening and supplies the cancellous bone and marrow. The epiphyseal artery separately enters the ends of long bones to supply the area, and periosteal arteries enter at numerous points to supply the compact bone. Veins exiting the bones carry blood cells to the body (Fig. 3-14). Primary ossification begins before birth and forms the entire bulk of the short and irregular bones. This process forms the long central shaft in long bones. During development only, the long shaft of the bone is called the diaphysis (Fig. 3-15, A). Secondary ossification occurs after birth when a separate bone begins to develop at both ends of each long bone. Each end is called the epiphysis (Fig. 3-15, B). At first, the diaphysis and epiphysis are distinctly separate. As growth occurs, a plate of cartilage called the epiphyseal plate develops between the two areas (Fig. 3-15, C). This plate is seen on long bone radiographs of all pediatric patients (Fig. 3-16, A). The epiphyseal plate is important radiographically because it is a common site of fractures in pediatric patients. Near age 21 years, full ossification occurs, and the two areas become completely joined; only a moderately visible epiphyseal line appears on the bone (Fig. 3-16, B).
GENERAL ANATOMY AND RADIOGRAPHIC POSITIONING TERMINOLOGY

General Anatomy
BODY PLANES
Sagittal plane
Coronal plane
Horizontal plane
Oblique plane
SPECIAL PLANES
Interiliac plane
BODY CAVITIES
DIVISIONS OF THE ABDOMEN
Quadrants
SURFACE LANDMARKS
BODY HABITUS
Osteology
GENERAL BONE FEATURES
BONE VESSELS AND NERVES
BONE DEVELOPMENT
Primary ossification
Secondary ossification
GENERAL ANATOMY AND RADIOGRAPHIC POSITIONING TERMINOLOGY