Presentation and Presenting Images
A 49-year-old female presents for screening mammography.
34.2 Key Images
34.2.1 Breast Tissue Density
There are scattered areas of fibroglandular density.
34.2.2 Imaging Findings
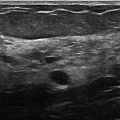
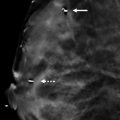
There is a group of calcifications in the right breast at the 9 o’clock location in the posterior depth. These calcifications are very faint and difficult to see on the digital breast tomosynthesis (DBT) images. In the area of the calcifications, the DBT does not reveal any associated mass.
34.3 BI-RADS Classification and Action
Category 0: Mammography: Incomplete. Need additional imaging evaluation and/or prior mammograms for comparison.
34.4 Diagnostic Images
( ▶ Fig. 34.5, ▶ Fig. 34.6, ▶ Fig. 34.7, ▶ Fig. 34.8, ▶ Fig. 34.9)
34.4.1 Imaging Findings
The diagnostic imaging demonstrates a 1.5-cm group of amorphous calcifications in the posterior depth at the 9 o’clock location. They do not layer on the lateral magnification view. There is no associated mass. These calcifications were sampled using stereotactic biopsy. Multiple cores contained the calcifications of interest.
34.5 BI-RADS Classification and Action
Category 4A: Low suspicion for malignancy
34.6 Differential Diagnosis
Flat epithelial atypia (FEA): FEA presents as grouped amorphous calcifications. By imaging, it is not discernable from any other cause for amorphous calcifications. Amorphous calcifications represent malignancy in 13 to 25% of biopsies. A biopsy is warranted. The fine nature of these amorphous calcifications may be at the limit of DBTs sensitivity in the reconstruction images.
Ductal carcinoma in situ (DCIS): DCIS has variable presentations. Low-grade DCIS is most commonly associated with amorphous calcifications.
Fibrocystic changes: Amorphous calcifications can be associated with cysts seen in fibrocystic changes.
34.7 Essential Facts
FEA is the term used when the epithelial layer of the duct is replaced by one to several layers of cuboidal to columnar cells with low-grade atypia.
Intraluminal secretions are common in FEA and have a tendency to calcify.
FEA is considered a high-risk lesion.
FEA is frequently associated with atypical ductal hyperplasia (ADH), lobular neoplasia, low-grade DCIS, and tubular carcinoma.
FEA is considered by many to be a precursor to low-grade DCIS.
Most recommend excision of FEA diagnosed at core needle biopsy.
Full-field digital mammography (FFDM) is more sensitive than DBT to the detection of calcifications.
34.8 Management and Digital Breast Tomosynthesis Principles
Slabbing of DBT slices (that is, combining slices, yielding a set of thicker images) may help in perceiving the distribution of calcifications.
The fineness of amorphous calcifications may limit their perception in the reconstructed DBT planes, thus the importance in calcification assessment of also obtaining a full-field digital mammogram (FFDM) or synthesized mammogram when DBT studies are obtained.
There is lack of data on the upgrade rates of FEA; there is controversy as to whether FEA is a precursor to low-grade DCIS or low-grade invasive carcinoma.
DBT’s viewing of images in slices may impede the perception of the distribution, or clustering, of calcifications.
There is limited literature on the evaluation of calcifications on DBT. Studies are needed to assess the observed morphology of calcifications on DBT and their benign or malignant outcomes.
34.9 Further Reading
[1] Molleran V. Postbiopsy management. Semin Roentgenol. 2011; 46(1): 40‐50 PubMed
[2] Spangler ML, Zuley ML, Sumkin JH, et al. Detection and classification of calcifications on digital breast tomosynthesis and 2D digital mammography: a comparison. AJR Am J Roentgenol. 2011; 196(2): 320‐324 PubMed

Fig. 34.1 Right craniocaudal (RCC) mammogram.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


