Blurring and widening of the margins of the physis. Osteopenia with resorption of trabeculae.
Deficient ossification of the zone of provisional calcification. Etiology is vitamin D deficiency, either acquired or congenital (malabsorption, failure of conversion to active form of vitamin D, renal osteodystrophy, etc.).
The epiphysis is separated and sometimes displaced from the metaphysis.
Distal humerus in infants and young children. Although the physis is typically narrowed in slipped capital femoral epiphysis, widening of the physis may occur in association with slippage of the epiphysis.
Metaphyseal chondrodysplasia
Several different types, some with known genetic deficiencies in either parathyroid hormone or collagen function.
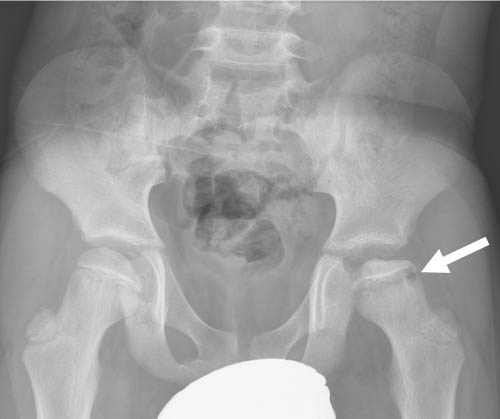
Fig. 5.63 Rickets. Renal osteodystrophy with diffuse bone demineralization and resorption.Fig. 5.64 Legg-Calvé-Perthes disease. In addition to the epiphyseal sclerosis the physis is widened (arrow).Fig. 5.65a, b Slipped capital femoral epiphysis (SCFI). The left physis is widened on the frontal projection (a) and SCFI is confirmed on the frog-leg view (b).
Table 5.40 Physis: narrowing and premature closure of the growth plate
Usually focal bone bridge (bar) with limb-length discrepancy ± angular deformity.
Frank destruction or local ischemia results in bridging after fracture or infection. Recruitment of osteoprogenitor cells via blood vessels that cross the physis may promote bone bridge formation. MRI may help quantify amount of bone bridge and direct treatment.
Advanced bone age
Normal architecture and mineralization.
All growth plates are affected similarly. A child’s current height and bone age can be used to predict adult height.
DD: prolonged elevation of sex steroid levels (precocious puberty or congenital adrenal hyperplasia), premature adrenarche, obesity from a young age, lipodystrophy, genetic overgrowth syndromes (Sotos, Beckwith-Wiedemann, and Marshall-Smith syndromes).
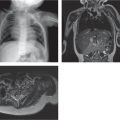
Fig. 5.66a–d Bone bridge formation after physeal injury. Acute Salter-Harris fracture (a) followed 1 year later by premature physeal closure on T1 (b) and DESS MRI (arrow in c). (d) Maximum intensity projection imaging from the DESS data quantifies the amount of bridging (area 3).
Only gold members can continue reading. Log In or Register to continue