Abstract
The head and neck have complex anatomy and there are multiple causes of physiologic FD avidity in the head and neck. Proper evaluation of benign and malignant lesions depends on knowledge of this anatomy and how it is altered by surgery, chemotherapy, and radiation.
Keywords
FDG, PET/CT, head, neck, thyroid, vocal cords, squamous cell carcinoma, lymphoma, orbit
Head and Neck Anatomy
The head and neck has complex anatomy. Proper identification of benign and malignant lesions depends on an understanding of this anatomy and how it may be altered by surgery, chemotherapy, and radiation.
The suprahyoid neck is divided by fascial planes into spaces. While the fascia is not visible on imaging studies, the spaces created by the fascia contain specific structures and the differential diagnosis of a lesion depends on which space the lesion is found in. Thus it is important to be able to localize a mass into one of the spaces. This can often be accomplished by concentrating on the parapharyngeal space (PPS; Fig. 7.1 ). The PPS contains mostly fat and is an uncommon site for abnormalities, but the fat in the PPS is displaced by masses in other spaces in characteristic directions ( Fig. 7.2 ).


When the PPS fat is displaced posterolaterally, the mass originates in the pharyngeal mucosal space. The pharyngeal mucosal space contains the naso- and oropharyngeal mucosa. Masses in the pharyngeal mucosal space are often malignant and most commonly include squamous cell carcinoma (SCC) of the naso- and oropharynx. Other differentials in the pharyngeal mucosal space include minor salivary gland tumors, lymphoma, and abscess.
When the PPS fat is displaced posteromedially, the mass originates in the masticator space. Masses in the masticator space are usually benign, most commonly dental infections. Other differentials in the masticator space include accessory parotid tissue and muscle hypertrophy. Malignancy in the masticator space is less common, but does occur.
When the PPS fat is displaced anteromedially, the mass originates in the parotid space. Masses in the parotid space are most commonly salivary gland tumors, both benign and malignant. Of course, lymphoma, metastases, and benign lesions from parotitis and sialolithiasis also occur.
And when the PPS fat is displaced anterolaterally, the mass originates in the carotid space. Carotid space masses are usually benign, most commonly paraganglioma and nerve sheath tumors. Of course, malignant lesions, such as nodal metastases, occur here.
Knowing the differential diagnoses based on neck spaces will help interpret imaging findings. While benign and malignant lesions are found in all spaces, a pharyngeal mucosal space mass should first raise concern for SCC, while masticator and carotid space masses should be recognized as most commonly benign. 18F-fluorodeoxyglucose (FDG)-avid foci along the mandible are examples of masticator space lesions which are usually benign dental inflammation.
Lymph nodes in the neck are commonly involved in head and neck malignancy. To help localize nodes and understand nodal drainage pathways in the head and neck, there is a commonly utilized system of nodal levels ( Fig. 7.3 ). Above the hyoid bone are found nodal levels I, II, and the superior portion of V. Level I is anterior to the posterior edge of the submandibular gland. Level V is posterior to the sternocleidomastoid muscle. Level II is between levels I and V, along the internal jugular vein, above the hyoid bone. Below the hyoid bone are found levels III, IV, VI, and the inferior portion of V. Level VI is medial to carotid arteries. Again, level V is posterior to the sternocleidomastoid muscle. Levels III and IV are between levels VI and V, with level III between the hyoid bone and the cricoid cartilage and level IV between the cricoid cartilage and the clavicle. Is takes some practice to properly classify nodes in this system, but it is worth it. Head and neck surgeons use the nodal levels to classify neck nodes; thus using this system will help you communicate with surgeons. Furthermore, primary head and neck SCCs drain to predictable nodal levels. For instance, pharynx cancers and supraglottic larynx usually drain to levels II to V, while infraglottic and thyroid cancers usually drain to level VI. Oral cavity cancers drain first to level I. Thus understanding the nodal levels will help you determine where to expect nodal metastases from head and neck squamous cell cancers.

Physiology FDG Avidity in the Head and Neck
There are multiple organs in the head and neck with physiologic FDG avidity. This makes comparison of FDG positron emission tomography (PET) images with the corresponding computed tomography (CT) images particularly useful in the head and neck. Localization of FDG avidity to an organ known to have physiologic FDG avidity, without a corresponding CT abnormality, is almost always benign.
Organs in the head and neck with physiologic FDG avidity include the salivary glands (parotid, submandibular, and sublingual glands) and the lymphoid tissue of Waldeyer ring ( Fig. 7.4 ). Waldeyer ring extends from the adenoids superiorly, and extends posterolaterally through the palatine tonsils to converge in the midline again at the base of tongue. The intensity of FDG avidity in these tissues varies among patients and may also vary between scans of a single patient. The intensity of avidity in any of these organs may range from background avidity to the most avid structure on the image, and any level of avidity may still be physiologic and benign. There may be left-right asymmetry in the level of FDG avidity in any of these organs from physiologic variation or caused by resection or radiation in one side of the neck.

Muscles of the head and neck may be avid (see Chapter 4 ). These include the muscles of mastication, the ocular muscles, and neck musculature. Curvilinear FDG avidity in muscles, without corresponding CT abnormality, is usually benign. More focal FDG avidity may require further evaluation with contrast-enhanced CT or magnetic resonance (MR) to exclude an underlying mass.
Brown fat may be FDG avid. It is called “brown” because of the more numerous pigmented mitochondria compared with typical “white” fat. These two types of fat have the same attenuation and are indistinguishable on CT. The CT component of the PET/CT is crucial for distinguishing brown fat from more ominous findings (see Chapter 21 ). Unless the patient has a very rare liposarcoma or malignant teratoma, the presence of fat can be a reliable sign that something is benign. FDG avidity in the neck that corresponds to fat on the CT is almost certainly benign brown fat. If the FDG avidity corresponds to soft tissue on CT, then brown fat can be excluded.
The tremendous variability in physiologic FDG avidity in the head and neck may make distinguishing FDG-avid malignancy from benign physiologic FDG avidity difficult.
Anatomic and Metabolic Alterations by Surgery and Chemoradiation
Surgery and chemoradiation may alter the physiologic FDG-avid structures in the head and neck. Identifying the surgical and chemoradiation changes in a scan will help prevent missing malignancy or misinterpreting a remaining physiologic structure as malignant.
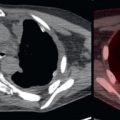
Neck dissections are a common surgical procedure in patients with SCCs of the head and neck. In addition to nodes, neck dissections may or may not include resection of additional structures, including the submandibular gland, sternocleidomastoid muscle, accessory nerve (cranial nerve XI), and/or internal jugular vein. Having an unpaired submandibular gland, due to resection of one in a neck dissection, could easily be mistaken for an FDG-avid node ( Fig. 7.5 ). Resection of a sternocleidomastoid muscle could lead to confusion in the contour of the neck ( Fig. 7.6 ) or if the remaining sternocleidomastoid muscle is FDG avid. The accessory nerve cannot be seen on CT; however, the effects of accessory nerve resection may still be identified. The accessory nerve innervates the trapezius and the sternocleidomastoid muscles. Atrophy of these muscles often helps identify an accessory nerve resection ( Fig. 7.7 ).



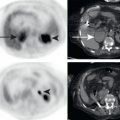
In addition to neck dissections, surgical resection of a primary malignancy may alter the appearance of normally FDG-avid structures in the head and neck ( Fig. 7.8 ). Resection of a salivary gland or tonsil may leave an unpaired FDG-avid structure that could be mistaken for a nodal metastasis. Following resection of a head and neck malignancy, the area may be reconstructed. Reconstructions with myocutaneous flaps may contain fatty elements, as well as muscle. The muscular component of flaps may have FDG avidity, which must be recognized as benign ( Fig. 7.9 ).


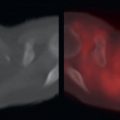
Chemotherapy and other systemic therapies may have side effects that may be FDG avid. One notable example is bisphosphonate therapy. Bisphosphonates help prevent bone resorption and may be used in patients with osseous metastases. Osteonecrosis of the mandible is a well-recognized side effect of bisphosphonate therapy ( Fig. 7.10 ). Radiotherapy may cause FDG-avid postradiation inflammation or may alternatively injure structures and decrease physiology FDG avidity. Salivary glands or lymphoid tissue in a radiation port may demonstrate reduced FDG avidity, and this may cause asymmetry in pair structures. Radiation may injure nerves, and this may lead to asymmetric FDG avidity in muscular structures. A known example is radiation injury to the hypoglossal nerve causing unilateral tongue FDG avidity ( Fig. 7.11 ).