Chapter 8 Heart
Methods of imaging the heart
ANGIOCARDIOGRAPHY
Indications
Equipment


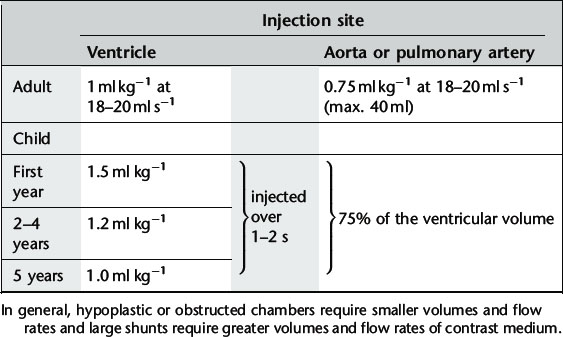
Technique
Image acquisition
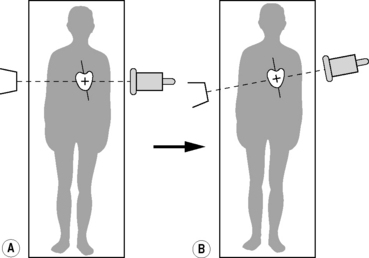
Using digital angiography at 30 frames s−1 with axial alignment of the heart, i.e. the X-ray beam is aligned perpendicular to the long axis of the heart (Fig. 8.4). The long axis of the heart is usually oblique to the long axis of the patient’s body and cardiac angiography suites have movable C-arms which allow correct positioning by movement of the equipment alone without disturbing the patient (Fig. 8.4b). Further rotation of the direction of the X-ray beam is used to profile those areas of the heart under examination. Useful views are:
CORONARY ARTERIOGRAPHY
Indications
Diagnostic arteriography can be supplemented by intravascular ultrasound (US) to determine the nature and extent of plaque within the vessel wall or angioscopy in some centres.
Equipment
Technique
The catheter is introduced using the Seldinger technique via the radial, brachial or femoral artery and advanced until its tip lies in the ostium of the coronary artery.
Image acquisition
Angiography (30 frames s−1) is performed in the following positions:
CARDIAC COMPUTED TOMOGRAPHY (INCLUDING CORONARY COMPUTED TOMOGRAPHIC ANGIOGRAPHY)
As a result of advances in CT technology, non-invasive cardiac imaging is becoming central to the diagnosis and management of patients with cardiac disease. This is the result of fast scan times and cardiac gating facilities available with multidetector CT scanners. Whilst the examination is tailored to assessment of the cardiac structures, CT imaging gives the benefit over conventional cardiac and coronary angiography of demonstrating clinically significant non-cardiac findings within the adjacent mediastinum, lungs or upper abdomen,1 and can give additional information regarding plaque characterization.
Cardiac CT may be performed as:
The coronary artery calcium (CAC) score is calculated from the volume of calcium present in the coronary arteries. A high score indicates an increased risk of adverse coronary events and CAC scoring has been used as a screening tool for subclinical cardiac disease. Absence of coronary artery calcification does not exclude atheroma but is associated with a low risk of adverse coronary event. Evidence shows that scores will probably need to be matched to age, sex and ethnic background.2
Coronary computed tomographic angiography
Documented mean effective radiation dose for coronary CTA ranges from 6 to 25 mSv3 and reported mean effective dose for conventional catheter angiography is 5.6 mSv.4 Further improvements in CT technology continue to reduce effective dose but there must be constant awareness with attempt to minimize dose wherever possible. Tailored coronary CTA is well-documented to have a high negative predictive value for coronary artery stenosis.5,6
Indications
Technique
The exact technique will depend on individual CT scanner technology and requires a multidetector CT which is 16 slice or above. Each CT manufacturer will advise scan protocols tailored to their specific scanners; however, general parameters useful for coronary artery assessment cardiac CT are as follows:7
1 Weinreb J.C., Larson P.A., Woodard P.K., et al. American College of Radiology clinical statement on noninvasive cardiac imaging. Radiology. 2005;235:723-727.
2 Preis S.R., O’Donnell C.J. Coronary heart disease risk assessment by traditional risk factors and newer subclinical disease imaging: is a ‘one-size-fits-all’ approach the best option? Editorial. Arch. Intern. Med.


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


