Key Points
- ▪
One of the great contributions of chest radiography to clinical cardiology and intensive care medicine is the assessment of left-sided heart failure, because chest radiography adds incrementally to the sensitivity and specificity of bedside physical diagnosis assessment of heart failure, especially in shock patients.
- ▪
There are distinct radiographic patterns of the permutations of acute and chronic left-sided and right-sided heart failure.
- ▪
The specific signs and stages of left-sided heart failure should be well understood.
Radiographic Patterns of Heart Failure
Clinically, it is useful to approach congestive heart failure as acute versus chronic and left-sided versus right-sided, because each has a specific differential diagnosis.
Acute Left-Sided Heart Failure
In acute left heart failure, the cardiopericardial silhouette (CPS) may be normal-sized or may be enlarged. In addition, there is the “butterfly” or “bat wing” pattern of acute pulmonary edema. These terms refer to the appearance of infiltrations extending from the hila, surrounded by radiolucent lung. Interstitial infiltrates are often most apparent over the hila; there, the interstitial septa are closest together. The interstitial septa radiate outward from the hilum because embryologically, the lung develops from the hilum outward.
Acute heart failure may develop in the case of a normal CPS (i.e., in the context of an acute infarction of a previously normal heart) or may develop in a heart that was previously diseased and enlarged.
The radiographic picture of acute left-sided heart failure is very similar to that of the adult respiratory distress syndrome (ARDS); in fact, the two often cannot be distinguished by chest radiography with sufficient confidence for clinical purposes. There is a tendency in ARDS for the infiltrations to begin in the periphery and extend centrally, whereas in heart failure, conversely, they tend to begin centrally and extend peripherally. There is also a tendency for the infiltrations of ARDS to be more diffuse than those of heart failure. In acute left heart failure the pulmonary veins are dilated.
Chronic Left-Sided Heart Failure
This condition is suggested by enlarged left-sided cardiac chambers, with evidence of pulmonary venous hypertension and with bilateral or a right-sided pleural effusion. (From 10% to 15% of patients with chronic left-sided heart failure have only a left-sided pleural effusion, which, being unusual, should prompt consideration of other causes of pleural disease.) Kerley B lines are common.
Acute Right-Sided Heart Failure
This condition usually occurs with an unremarkable CPS, but it may show progressive right-sided enlargement and dilatation of the azygous vein. Look for signs of pulmonary embolism, which is a common cause of acute right-sided heart failure.
Chronic Right-Sided Heart Failure
Note overaeration of the lungs, decreased lung vascularity, centralization of flow, and CPS enlargement.
Pulmonary Edema
The following categories are “idealized” but useful for their pathophysiological approach.
Stage 1: Increased Fluid Formation, Increased Removal
This stage is characterized by the following:
- □
No net accumulation
- □
Increased resistance to flow to the base (the arteries and veins to the lower lobes are compressed by perivascular edema), resulting in increased flow to the apices. This leads to “redistribution” (the vessels to the apex are larger than those to the base). Redistribution is an applicable sign only in erect views and is the earliest sign of pulmonary venous hypertension.
Stage 2: Interstitial Edema ( Fig. 6-1 )
This stage is characterized by the following:
- □
Fluid accumulation in the interstitial spaces (perivascular sheaths, interlobular septa, subpleural spaces, bronchial walls [peribronchial “cuffing”], and between fissures) ( Figs. 6-2 to 6-4 )

Figure 6-2
The cardiothoracic ratio and contours of the cardiopericardial silhouette are difficult to assess due to obscuring of the borders of the heart by interstitial and airspace pulmonary edema and also superimposition of breast shadow. There is acute pulmonary edema due to hypertensive crisis in a patient with left ventricular hypertrophy and normal systolic function. Note the severe calcification of the abdominal aorta apparent best on the lateral view, a contributor to the systolic hypertension by rendering of the aorta extremely noncompliant.

Figure 6-3
Anteroposterior chest radiograph. The cardiothoracic ratio is increased without particular contour abnormality. There is rotation of the chest. There are both interstitial and airspace pulmonary edema with obscuring of the hilar structures resulting in the “bat wing” pattern. The aorta is heavily calcified at the arch level. There is acute pulmonary edema due to hypertensive crisis in a patient with systolic hypertension, left ventricular hypertrophy, and normal systolic function.

Figure 6-4
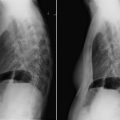
Posteroanterior and lateral chest radiographs. There is congestive heart failure due to cardiomyopathy. Pleural effusions are typical of chronic biventricular heart failure. Due to the presence of significant size bilateral pleural effusions, the cardiothoracic ratio and the cardiopericardial contours cannot be assessed. There is extensive interstitial pulmonary edema and increased pulmonary venous prominence.
- □
Hazy hila ( Fig. 6-5 ). Embryologically, the lung parenchyma grew out from the hila. The pulmonary septa therefore radiate away from the hilum and are closest together at the hila and farthest apart at the pleural surface. Accumulation of septal edema therefore is most apparent at the hila, where the septa converge.

Figure 6-5
Severe bilateral airspace and interstitial pulmonary edema, most apparent over the hila. The cardiac silhouette is nearly impossible to interpret due to rotation, poor inspiration, and silhouetting of the heart by the pulmonary edema.
- □
Interstitial edema/infiltrates that render the right lower pulmonary artery indistinct
- □
Common Kerley B lines (see later discussion)
- □
Thickened interstitial spaces with pulmonary edema that are indistinct (whereas those due to lymphangitic cancer and to pulmonary fibrosis may be better defined)

Stage 3: (Intra-)alveolar Edema
This stage is characterized by alveolar or intra-alveolar edema, which appears as puffy 2 to 3 mm round or confluent opacities.
Stage 4: Hemosiderosis plus Ossification of Lung
This stage is characterized by the following:
- □
Hemosiderosis and ossification of the lung that occur as an airspace pattern with a “stippled” appearance due to multiple nodules. This is an uncommon finding of very severe mitral stenosis with repeated episodes or pulmonary edema and hemorrhage.
- □
Differential diagnosis: prior granulomatous disease, calcified metastases (e.g., osteosarcoma)
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


